
CDC Ignores Cold Turkey Quitters
Government health policymakers continue to give millions of cold turkey quitters the cold shoulder despite the plea of tobacco control's leading integrity watchdog, Professor Michael Siegel of Boston University School of Public Health, and the "elephant in the room" analysis of the former editor of the leading tobacco control journal, Simon Chapman, Professor of Public Health at the University of Sydney. Below is an open letter to the U.S. Centers for Disease Control's (CDC) senior quit smoking scientist from the director of the Internet's leading cold turkey quit smoking forum.
Terry F. Pechacek, PhD
Associate Director for Science
Office on Smoking and Health
Centers for Disease Control
1600 Clifton Road, Atlanta, Georgia 30333
Email: txp2@cdc.gov
Re: Plea that the CDC motivate, educate and support cold turkey quitters
Dear Dr. Pechacek,
As you know, during 2010 cold turkey will account for more long-term successful quitters than all other quitting methods combined. As senior scientist at the CDC's Office on Smoking and Health (OSH) since 1999, America's lead agency in the war against tobacco induced disease and death, I write imploring OSH to immediately reverse course and end the practice of undermining and discouraging cold turkey quitting attempts, to at last begin supporting their efforts.
Dr. Pechacek, OSH is guilty of having taken its eye off the ball. Its mission statement makes it nicotine dependency recovery's integrity guardian, as even the tobacco industry acknowledges that nicotine is the sine qua non of smoking. With due respect, OSH has failed horribly.
If a certain strain of flu was killing 400,000 Americans annually, would the CDC continue to make failed medicines the cornerstone of treatment?  How many millions more must die before OSH demands re-examination of our nation's quitting policy?
How many millions more must die before OSH demands re-examination of our nation's quitting policy?
As you know, since June 2000, official U.S. smoking cessation policy, as reflected in the PHS Clinical Practice Guideline for Treating Tobacco Use and Dependence, has effectively outlawed any government support of smokers attempting to quit cold turkey. "There are numerous effective medications for tobacco dependence," it proclaimed, "and clinicians should encourage their use by all patients attempting to quit smoking."
Authored by an expert panel having heavy pharmaceutical industry financial ties, their blanket medication recommendation effectively consumed all other recommendations, destroyed government support for cold turkey quitters and quitting, medicalized cessation, guaranteed massive profits to the pharmaceutical industry, and has since resulted in thousands of needless deaths as cessation stalled and has been brought to its knees.
As the nation's primary tobacco control guardian, it was OSH's duty to investigate, question and expose financial conflicts among "experts" invited to author official U.S. quitting policy. On February 8, 2007, we awoke to front page Wall Street Journal headlines blasting U.S. health officials for allowing pharmaceutical influence to coin policy while undermining cold turkey quitting.
OSH was given a second chance at restoring policy integrity during 2007-08 when the U.S. Guideline underwent revision to incorporate Pfizer's new stop smoking pill Chantix. Again, revised findings were soaked in pharm influence, as at least nine panel members had industry financial ties.
Plea to Amend U.S. Cessation Policy
Dr. Pechacek, below are current 2008 U.S. Guideline panel findings in need of immediate amendment, each fully supported by the existing evidence base. If adopted, they would empower U.S. health agencies and clinicians to end discrimination against cold turkey quitters, and openly provide them with encouragement, counseling, education and support.
CURRENT RECOMMENDATION 6: "There are numerous effective medications for tobacco dependence and clinicians should encourage their use by all patients attempting to quit smoking, except when medically contraindicated or with specific populations for which there is insufficient evidence of effectiveness (i.e., pregnant women, smokeless tobacco users, light smokers and adolescents)."
 RECOMMENDED AMENDMENT: "While evidence of real-world effectiveness has not yet been demonstrated, numerous FDA approved stop smoking products have demonstrated clinical efficacy in placebo controlled trials and may be used by patients attempting to quit smoking, unless medically contraindicated or within specific populations for which there is insufficient evidence of efficacy (i.e., pregnant women, smokeless tobacco users, light smokers and adolescents)."
RECOMMENDED AMENDMENT: "While evidence of real-world effectiveness has not yet been demonstrated, numerous FDA approved stop smoking products have demonstrated clinical efficacy in placebo controlled trials and may be used by patients attempting to quit smoking, unless medically contraindicated or within specific populations for which there is insufficient evidence of efficacy (i.e., pregnant women, smokeless tobacco users, light smokers and adolescents)."
CURRENT RECOMMENDATION 3: Tobacco dependence treatments are effective across a broad range of populations. Clinicians should encourage every patient willing to make a quit attempt to use the recommended counseling treatments and medications in the Guideline.
RECOMMENDED AMENDMENT: While evidence of real-world effectiveness has not yet been demonstrated, FDA approved stop smoking products have demonstrated clinical trial efficacy over placebo controls across a broad range of populations. While clinicians should encourage patients willing to make a quit attempt to use counseling, support or approved products identified in the Guideline, quitters expressing desire to quit without counseling, support or product use should be encouraged and supported in their quest.
Also, Dr. Pechacek, evidence supporting Recommendation 7 is extremely weak. The focus of most counseling within clinical trials has centered on proper quitting product use. While little quality evidence exists contrasting non-pharm counseling and support programs to product use alone, there is strong evidence of dismal cessation rates when products are used without counseling or support. Current Recommendation 7 is yet another means by which "medicine" recommendations totally consume counseling and support.
CURRENT RECOMMENDATION 7: Counseling and medication are effective when used by themselves for treating tobacco dependence. However, the combination of counseling and medication is more effective than either alone. Thus, clinicians should encourage all individuals making a quit attempt to use both counseling and medication.
RECOMMENDED AMENDMENT: Counseling and approved product use have shown clinical efficacy when used by themselves for smoking cessation. However, the combination of counseling and product use has shown greater efficacy than product use alone. Thus, clinicians should encourage all individuals making a quit attempt while using approved products to supplement product use with counseling.
I would also encourage the OSH to support new recommendation 11:
RECOMMENDATION 11: Unassisted quitting continues to account for more successful long-term ex-smokers than all other quitting methods combined. Quality research into how unassisted quitters succeed has been seriously neglected. Most real-world quitting method surveys continue to suggest long-term unassisted quitter success rates comparable or superior to FDA approved quitting product use alone. Clinicians should offer those wishing to quit cold turkey or unassisted as much support, non-pharmacotherapy counseling and relapse prevention instruction as they are willing to accept.
"Best Practices" and "Healthy People" Goals
OSH boasts a 145 member staff and a $100 million annual budget. Sadly, not one employee or one dollar will be devoted during 2010 toward improving, promoting and supporting cold turkey quitting. It isn't by chance or oversight but policy. Why?
Dr. Pechacek, since 1999 you've served as lead author of the CDC's "Best Practices" for successful quitting. On what occasions have you questioned pharmaceutical influence in authoring official policy, or challenged the placebo-controlled science supporting it?
Instead, your "Best Practices" cessation recommendation simply parrots the PHS Guideline in asserting that all tobacco users should receive "FDA-approved cessation medication."
The CDC's 1998 "Healthy People 2010" goal was to reduce the adult smoking rate from 24% in 1998 to 12% by 2010 [Note: the new Healthy People 2020 adult smoking objective is to reduce smoking from 20.6% in 2008 to 8% in 2020].
Today, after a decade long mandatory "medicine" use policy that promised to at least double quitting rates, after significant tax related cigarette price increases, substantial societal restrictions on when and where smokers can smoke, the systematic erosion of smoker self esteem that's left them with elevated anxieties and feeling like social outcasts and lepers, the adult smoking rate is 21%.
Having failed miserably and the annual death toll hovering near half a million, one would think that CDC leadership would demand an emergency policy review, get to the bottom of things, and that heads would roll. Instead, OSH's annual smoking survey data reviews (MMWRs) seem to blame everyone and everything except internal CDC cessation policy. The "Editorial Note" to OSH's latest survey findings dated November 13, 2009 blames cultural factors, low educational levels, and under-funding of "treatment."
Imagine the relapse mess the CDC would foster if it spent the next decade teaching alcoholics that intravenously administered replacement alcohol was "medicine" and its use "therapy." That's exactly the course taken with replacement nicotine.
Like pouring mud in a swimming pool, the CDC and OSH made it vastly more challenging for nicotine addicts to see and self-discover the most critical quitting lesson of all via the school of hard-quitting-knocks, the Law of Addiction. It states, "Administration of a drug to an addict will cause re-establishment of chemical dependence upon the addictive substance."
As you know, just one puff and up to 50% of the brain's a4b2-type nicotinic receptors become occupied by nicotine. While most walk away from relapse thinking they've gotten away with using, a powerful nicotine induced dopamine explosion has awakened their dependency, and their brain will soon be begging for more.
Why did OSH remain silent as pharmaceutical industry consultants masquerading as independent researchers compared and equated the performance of someone who has ended all nicotine use, to someone still using? Why remain silent as all who became chronically dependent upon the cure, including President Obama, were hailed as successful quitters? Why doesn't any OSH webpage document nicotine's known harms?
Imagine the intellectual dishonesty it took to pretend during more than 300 placebo-controlled studies that smokers with significant quitting histories were not experts at immediately recognizing the onset of their withdrawal syndrome after randomization to the placebo group. Dr. Pechacek, you must know by now that the use of placebo controls in drug addiction studies is license to steal, that assignment awareness among experienced quitters should be expected within 24 to 48 hours of cessation.
Name any other study area where the condition sought to be treated (withdrawal) does not exist until researchers say, "ready, set, go!" Name any other study area where the placebo group is punished with the onset of powerful anxieties and made vastly worse than when they arrived. Enticed to join the study by a promise of "free medicine," frustrated by placebo assignment awareness, how many grew frustrated, threw in the towel, and helped hand the active intervention victory by default?
Dr. Pechacek, your own 1991 self-help study found that 10% of non-medication quitters were still not smoking at 7 months. Where was your voice when the meta-analysis of NRT product use under over-the-counter conditions reported a 7% NRT quitting rate at six months, while the placebo group's six month rate was astonishingly low at just 3%, three times lower than your 10% finding?
While industry consultants want us to believe that the remaining 21% of the population still smoking reflects hardened and more dependent smokers, I submit they are simply confused, have been lied to, and neglected.

Why hide the National Cancer Institute's 2006 quitting method survey which found higher long-term success rates for non-medication quitters? Why suppress the fact that nearly every long-term real-world quitting method survey to date has found that those quitting without medications prevail over those who use them?
Abrupt Nicotine Cessation Science Challenge
Quitting cold turkey does not mean quitting in ignorance, darkness and unsupported. Traditionally it meant abrupt cessation of smoking, without use of products or procedures.
Dr. Pechacek, attached is a copy of Joel Spitzer's free e-book entitled "Never Take Another Puff." As you may know, having started as a teenage volunteer with the American Cancer Society, Spitzer has devoted nearly four decades, full-time to helping free smokers. America's Baby Ruth of quitting, his recovery insights are a national treasure.
As the CDC's senior smoking cessation scientist I challenge you to rip Spitzer's lessons apart, identifying any not rooted in rock solid abrupt nicotine cessation science. If unable to do so, what reason could you possibly have for not hosting Joel's free book and 64 video quitting lessons on OSH's CDC-based website?
If we're to get U.S. cessation back on track it will require a campaign to restore quitter confidence in their natural recovery instincts. As you know, 40% of adult smokers will make a serious attempt this year. It isn't that they don't want to stop but that their government refuses to teach them how. Why continue to deprive quitters of awareness of the most critical recovery lesson of all, that just one puff of nicotine when quitting and relapse is all but assured?
If knowledge is power then what learning takes place by swallowing a pill, slapping on a patch, chewing gum or sucking on a nicotine lozenge?
Although rooted in chemical dependency, with profound changes in brain physiology (receptor desensitization and up-regulation), the greatest portion of recovery remains psychological in nature. It's why attempts to medicate beliefs, conditioning, emotions, and use rationalizations was destined to flounder.
How do successful cold turkey quitters succeed? Isn't it time for the CDC to stop pretending that the keys to successful abrupt nicotine cessation is not rooted in knowledge, understanding, skills, support and science?
Is it realistic to expect profit driven corporations to support a free quitting method from which they cannot profit? Unless government assumes responsibility for investigating, protecting and sharing the abrupt cessation science base, we should fully expect the economic muscle of all seeking cessation product market share to hide, suppress and defame it.
Abrupt Nicotine Cessation Support Challenge
OSH's refusal to defend and support our nation's most productive quitting method has compelled others to do so. Constant questioning of the science underlying cessation via chemicals that continue dopamine stimulation instead of ending it, and an unwillingness to adhere to the June 2000 PHS Guideline's medication recommendation has caused the U.S. Public Health Service to view and treat site's like WhyQuit as the enemy. They're anything but.
 As evidenced for more than a decade, our volunteers do not need the CDC's or OSH's seal of approval. What we do need is for OSH to end the insanity of turning its back on the millions of U.S. smokers who this year will attempt to quit cold turkey.
As evidenced for more than a decade, our volunteers do not need the CDC's or OSH's seal of approval. What we do need is for OSH to end the insanity of turning its back on the millions of U.S. smokers who this year will attempt to quit cold turkey.
National telephone quit-lines continue to strongly push "medicine" while telling nearly all who call that without it their odds of failure double. Frankly, they continue to do so because that's what you're teaching them.
Dr. Pechacek, I watched your November "Public Health Grand Rounds" presentation addressing smoking cessation. I must say, I swallowed hard as you taught your audience that "very few of these unaided quit attempts are successful" and then showed a chart suggesting that medication triples quitting rates.
Why didn't you show them a chart like this instead? It's from data in a 2006 Australian study that followed smoking patients of family practice physicians and found that cold turkey quitters accounted for 1,942 of 2,207 former smokers, a whopping 88% of all success stories.
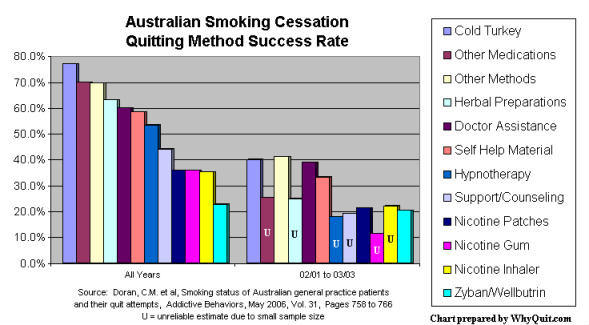
Until willing to admit to yourself that out here in the real-world medication does not double or triple success rates, that cold turkey remains king of the hill, you will continue to damage quitter trust and confidence in our nation's most productive quitting method.
It is time for OSH to do more than attempt to coerce cessation. In 1979 you wrote, "we have only begun to clarify how and why the average person succeeds or fails in attempts to become an ex-smoker." It's as if replacement nicotine's arrival in 1982 destroyed the quest to discover how nicotine addicts succeed in arresting their dependency.
Clearly, your instincts are correct, that social cognitive theory is key to affecting personal change. What's missing isn't theory or structure but identification of the knowledge, skills and behaviors needed to make dreams come true. Today, cessation product marketing actually undermines those dreams by painting non-product quitting as nearly impossible.
The CDC needs to develop its own online cold turkey quitting forum. It needs to demand review of national telephone quit-line counselor training and counseling scripts to ensure that counselors are supporting these quitters, not demoralizing them.
As you know, the support needs of cold turkey and medication quitters are as different as night and day. Cold turkey quitters experience peak physical withdrawal within 3 days. Receptor re-sensitization and down-regulation is believed substantially complete within 21 days. After that it's primarily a matter of relapse prevention. This mandates up-front education rich and support intense programs that aid quitters in navigating and moving beyond withdrawal.
Dr. Pechacek, it is OSH's health responsibility to orchestrate creation and deployment of the most effective cold turkey quitting tools smokers have ever seen, including high quality support. While true that roughly 10-12% of unassisted cold turkey quitters currently succeed in quitting for 6 months, how much improvement would be seen if OSH used low cost Internet based programs and existing telephone quit-lines to motivate, educate and support abrupt nicotine cessation? How will it know unless it tries?
Sincere regards,
John R. Polito
Nicotine Cessation Educator
106 Aldrich Place
Goose Creek, SC 29445
Email: john@whyquit.com
I, John R. Polito, am solely responsible for the content of this article. Any errors brought to my attention will be immediately corrected.

