
Is pregnancy NRT use worse than smoking?
The parade of studies fingering nicotine as tobacco's primary culprit in damaging normal fetal development during pregnancy continues. The newest study, soon to be published in the "Maternal and Child Health Journal," leaves smoking women, their physicians and researchers scratching their heads.
The study found that compared to both smokers and non-smokers, pregnant women that were recommended or prescribed the use of nicotine replacement products such as the nicotine patch, gum, lozenge, spray and inhaler (NRT) had increased risk of giving birth to a low birth weight baby and increased risk of not carrying to full term.
Surprisingly, pregnant women using NRT had a 95% increase in the odds of giving birth to a low birth baby weight baby (less than 5.5 pounds or 2500 grams) over women who did not smoke or use NRT. A frightening thirty-seven percent of all suspected NRT users gave birth to low birth weight babies (84 of 225 births) .
In contrast, women who continued smoking during pregnancy had a 31% increase in odds of giving birth to a low birth weight baby over women not using any form of nicotine. Still, in actual percentages, thirty-two percent of nicotine smokers gave birth to low birth weight babies (205 of 637 births) .
Normal full-term pregnancy is considered to be 40 weeks from the date of the start of a woman's last menstrual period, even though conception does not occur until two weeks later. Using 40 weeks, preterm birth is defined as any birth prior to 37 weeks.
According to the study, "Women prescribed or recommended NRT had twice the risk of preterm birth, and smokers had 1.09 times the risk of preterm birth as compared to nonsmokers."
Were women who used NRT during pregnancy somehow falsely led to believe that pharmaceutical nicotine was safe? Did such assurances of safety cause them to ingest significantly greater quantities of nicotine than if still smoking? We don't yet know.
Although noting that the U.S. Food and Drug Administration (FDA) classifies nicotine as a category D drug, and that animal studies have proven nicotine to be a powerful neuroteratogen which damages normal fetal development, the authors were at a loss to explain their findings, and could only offer speculation as to a number of possibilities.
A rash of recent studies suggest that smoking women with dreams of motherhood would be wise to arrest their chemical dependency now, prior to conception, as new evidence suggests that serious damage to the developing fetus likely begins far earlier than previously thought.
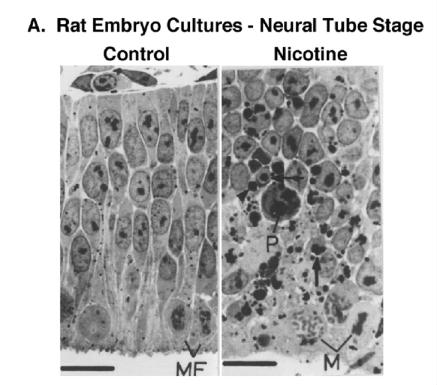 In January, Professor Theodore A. Slotkin, a Duke Medical University toxicologist, authored a disturbing review of the destructive impact of fetal and adolescent nicotine upon the developing animal brain. It described how nicotine hijacks and alters the trajectory of normal brain development. His slides show cellular damage inflicted by nicotine in the neural tube stage in rats, the embryotic stage during which the brain first begins to unfold, a stage that starts in human embryos within 3 to 4 weeks of conception.
In January, Professor Theodore A. Slotkin, a Duke Medical University toxicologist, authored a disturbing review of the destructive impact of fetal and adolescent nicotine upon the developing animal brain. It described how nicotine hijacks and alters the trajectory of normal brain development. His slides show cellular damage inflicted by nicotine in the neural tube stage in rats, the embryotic stage during which the brain first begins to unfold, a stage that starts in human embryos within 3 to 4 weeks of conception.
Entitled "If nicotine is a developmental neurotoxicant in animal studies, dare we recommend nicotine replacement therapy in pregnant women and adolescents," Slotkin asserts that "the cost of tobacco-related developmental damage includes immediate perinatal events, such as spontaneous abortions, intrauterine growth retardation and perinatal deaths, and Sudden Infant Death Syndrome. He reminds us that nicotine's consequences extend much further, encompassing subsequent learning disabilities, cognitive dysfunction, behavioral problems, attention deficit hyperactivity disorder, psychiatric disorders, conduct disorders, criminal behaviors and school and career failure."
It has long been known that the nicotine molecule mimics and imitates the neurotransmitter acetylcholine by attaching to and activating certain types of acetylcholine receptors. Slotkin teaches how nicotine disrupts normal brain development by activating acetylcholine receptors prematurely and with inappropriate intensity, before the brain neuron the receptor is attached to has had an opportunity to fully develop and properly interface with surrounding brain neurons.
Professor Slotkin expresses deep concern that the medical community has failed to "recognize the magnitude of the problem" or champion effective countermeasures in coming to the defense of healthy and natural fetal development.
In that nicotine is a potent neurotoxicant that adversely effects brain development and synaptic function, Slotkin is troubled by those advocating that expectant mothers or youth use nicotine replacement products (NRT). He argues that prior to making such recommendations proponents should have to prove that doing so is not only both safe and effective, but more effective than quitting without pharmacology.
Slotkin cites studies showing that NRT has not proven effective in either group. One NRT pregnancy study actually had to be discontinued after a 50% increase in adverse birth and neonatal outcomes. In a smaller study, 3 out of 21 infants showed severe neonatal morbidity and in another NRT increased the rate of congenital malformations.
While a number of harm reduction activists continue to falsely portray nicotine as being no more harmful than caffeine, Slotkin points to the fact that, "a number of animal studies of environmental tobacco smoke exposure, both in rodents and primates, point to virtually identical outcomes to those seen with nicotine alone." Those harms include neuronal and synaptic damage, cognitive dysfunction, adverse lung development, immune function and cardiorespiratory function.
Could nicotine delivered via NRT actually be more harmful to the fetus than smoking? According to Professor Slotkin, "there is abundant evidence that the major problem for fetal development is exposure to nicotine rather than other components of cigarette smoke."
Worse than smoking? Unless the expectant mother delivers a greater quantity of nicotine into her bloodstream than by smoking, probably not. But there is one delivery device causing concern, the nicotine patch.
"NRT, especially by transdermal patch, delivers more nicotine to the fetus than smoking does." According to Dr. Slotkin, a recent study found that the brains of fetal mice were found to have 2.5 times higher nicotine concentrations than found in the mother's blood when a slow continuous nicotine feed, as would be the case with the nicotine patch. It is believed that placenta nicotine filtering may somehow be overwhelmed by the steady stream introduced via the patch.
Although Slotkin never once challenges the motivations of those advocating NRT use during pregnancy, or by adolescent smokers, it is no secret that many of the most visible and vocal proponents have openly and repeatedly acknowledged financial ties to GlaxoSmithKine or Pfizer, the primary pharmaceutical companies involved in the sale of NRT products.
So how does the expectant woman quit? Key to breaking nicotine's grip is knowledge and understanding. Escape can be rather challenging if we have little understanding of where we reside and our chemical captor keeps us enslaved. Visit and explore WhyQuit if ready to have children or pregnant. The site is loaded with nicotine dependency recovery tools, staffed entirely by volunteers, sells nothing and actually declines donations. Ready for freedom from nicotine? Yes you can!
