
Little communication in failed war against smoking
The war against America's leading cause of preventable death has ground to a standstill. Hundreds of millions of precious tax dollars spent trying to counter tobacco industry marketing, while cigarette prices shot through the roof and clean indoor air laws swept the nation, and still only a modest 23 to 21 percent decline in the adult smoking rate over the past decade. Now, a new study reports that agency turf wars and a lack of time kept key tobacco control government health officials from communicating with each other.
 According to the August Tobacco & Nicotine Research journal study, eleven federal agencies within the U.S. Department of Health and Human Services (HHS) are charged with battling tobacco related dependency, disease and death. The study identified 54 tobacco policy, practice and research employees within those agencies as key tobacco control players. Forty-nine of them agreed to participate in the study's 2005 survey.
According to the August Tobacco & Nicotine Research journal study, eleven federal agencies within the U.S. Department of Health and Human Services (HHS) are charged with battling tobacco related dependency, disease and death. The study identified 54 tobacco policy, practice and research employees within those agencies as key tobacco control players. Forty-nine of them agreed to participate in the study's 2005 survey.
These 49 movers and shakers were questioned via e-mail about their communications and contacts within the HHS tobacco control network, and about barriers, if any, to effective inter-agency communication. Shockingly, some federal agencies reported little or no interaction with other agencies.
Picture America having 54 generals in a war that annually produces more than 400,000 deaths and, as reported by this study, 80% of our generals claiming that they don't have time to communicate with each other.
Tobacco network key employees at the Food and Drug Administration, which oversees quitting product approval, reported zero contacts with network employees within the other ten agencies. This despite growing concerns that use of placebo controls within nicotine replacement studies were not blind as claimed, and produced findings unworthy of belief.
The study also reported no inter-agency network contacts between the Centers for Medicare and Medicaid Services, which oversees payment for smoking cessation counseling. Additionally, extremely limited network interface was found at the Substance Abuse and Mental Health Services Administration, where the #1 objective is prevention of substance abuse.
According to the study, the Centers for Disease Control's (CDC) Office of Smoking and Health (OSH) is the most active agency in the war against smoking. What wasn't noted is that being active has not translated into effectiveness.
Among surveyed CDC network employees, 82% blamed failure to collaborate with other HHS agencies on a lack of time, 73% blamed bureaucracy, while 36% blamed inter-agency politics. Inside the National Institute of Health (NIH), home to the National Cancer Institute (NCI) and the National Institute on Drug Abuse (NIDA), 87% blamed time, 47% bureaucracy and 47% politics.
HHS's Failure to Protect Teens
The recent coal mining and Gulf drilling disasters suggest that when it comes to federal regulatory oversight that either the fox was in the hen house or the farmer was amazingly stupid. Sadly, in no hen house is the price of government ineptitude greater than in tobacco control's.
Here, the tobacco and pharmaceutical industries appear to rely heavily upon health bureaucrat time constraints, communication isolation and inter-agency turf wars in preying upon youth immaturity and quitter ignorance.
Imagine President Obama being complicit in allowing 350,000 kids to become trapped below ground in coal mining disasters, the number of new daily youth smokers this year.
Picture 443,000 dead nicotine addicts floating face down in the Gulf of Mexico, with hundreds of toxin and carcinogen filled bodies daily washing up on Texas and Florida beaches, yet no Presidential press conference, and no Presidential butt kicking.
U.S. tobacco prevention and cessation policy is an ignored national disaster. In fairness, incompetent tobacco control leadership within HHS should have been fired long before Obama's arrival.
Even so, is it reasonable to expect a President whose brain is itself slave to nicotine to declare and vigorously prosecute war against those supplying his drug, or to dismiss incapable health bureaucrats who congratulate him on having successfully quit?
Claiming "I am 95% cured" while mixing intermittent smoking relapses with chronic ongoing nicotine gum use since February 2007, arguably, no president in history has done more to muddy adolescent understanding of nicotine dependency than President Obama.
According to Dr. Nora D. Volkow, Director of the National Institute on Drug Abuse - possibly HHS's boldest and brightest thinker - nicotine addiction is a permanent disease and mental illness for which there is no cure. And while the dependency can be fully arrested, the recovered addict remains subject to relapse for the balance of life.
The President's own ongoing struggle has been a golden yet missed opportunity to teach youth that nicotine is extremely addictive. Up to 26 percent of adolescents exhibit signs of loss of control over continued smoking after just 3 to 4 cigarettes, rising to 44 percent after 5 to 9.
Nicotine quickly activates, saturates and desensitizes brain dopamine pathway receptors, which is followed by growth and activation of millions of extra receptors, a nicotine tolerance re-wiring process known as up-regulation.
The birth of a true dopamine "wanting" disorder that leaves the brain craving nicotine as though hungry or starving for food 5 to 60 times per day, nicotine dependency is as permanent as alcoholism, hijacks the same brain dopamine pathways as illegal drugs, and may be harder to beat than heroin.
HHS's Failure to Insulate Youth
The tobacco industry spends at least $12 billion annually to transform more than 140,000 neighborhood convenience stores into youth nicotine addiction traps. It knows that roughly two-thirds of teens are convenience store shoppers.
Most convenience stores make it impossible for a teen to purchase candy, chips or a soda without their subconscious mind being bombarded by scores of subliminal tobacco use invitations. A massive wall of brightly colored packs, cartons, cans, pouches and tubes all but wraps itself around them as they make their purchase. This contrived facade screams that tobacco use is normal, it's what adults do, it's flavorful and fun.
The store's intentional and well orchestrated assault pounds home the message that the student has not yet tasted life's best flavors, experienced real excitement, felt true pleasure, made enough friends, worn spurs, taken sufficient risk, rebelled or looked adult, until they've experimented with smoked or oral tobacco.
Preying upon immature minds that can't wait to be grown-ups, the industry knows that up to 90% of new smokers start prior to age 20. It knows that unless it chemically enslaves them while young and gullible that profits will nose dive.
The industry wants adults to believe that the giant yellow "We Card" signs are there to alert students that the store checks I.D.'s. But once secret tobacco industry documents suggest that they are another subconscious tease, a constant and intentional reminder to children and teens that smoking is a rite of passage into adulthood.
Common sense suggests that the President's army of health officials should be joining forces, communicating and working overtime in support of national, state and local laws designed to insulate youth from these highly effective marketing traps. It simply isn't happening.
The CDC's "Best Practices for Comprehensive Tobacco Control Programs 2007" is its cornerstone prevention policy document. Not once does this 122 page battle plan recommend passage of laws that would forbid youth under eighteen from entering tobacco sales locations, nor suggest amendment of local zoning ordinances so as to require removal of exterior store tobacco marketing signs, signs bombarding young minds in passing vehicles and school buses.
Instead of placing legislative barriers between youth and tobacco marketing, the CDC claims that the best way to protect students is to go toe-to-toe with industry advertising, by conducting expensive "counter-marketing strategies that employ a wide range of efforts, including paid television, radio, billboard, print, and web-based advertising at the state and local levels."
Under the CDC's failed slug it out policy, 26 percent of high school 12th graders smoked cigarettes in 2003 and an identical 26 percent were smoking four years later in 2007.
The tobacco industry also has a sick history of purchasing cigarette placement and use in P and PG rated movies, with smoking by heroes in recent movies being 3 to 4 times more likely than in real life.
Highly skilled at collecting and sharing facts, the CDC's web site warns that the average teen is exposed to 15 smoking scenes in moves per week and that "a teen whose favorite star smokes is significantly more likely to be a smoker." The CDC then turns yellow and wimpish in failing to propose a solution.
The government could push for R ratings or at least demand parental disclosure of tobacco use in all movie advertising in which any movie portrays smoking in a positive light. Instead, as with its failure to advocate insulating youth from store marketing, government health officials fear making waves, and present no plan for protecting them.
Imagine going to work each day and staring into the face of a youth to grave nicotine addiction pipeline that annually kills hundred of thousands, and then behaving like cowards afraid to fight. America's youth might be better off being protected by General Electric, Colonel Sanders and Captain Crunch.
Yes, passage of laws excluding youth from entering tobacco sales locations would be expected to diminish profits in those stores continuing to sell tobacco. But whether recognized and wanted or not, the decision to advertise and encourage the purchase and use of what may be the planet's most addictive substance should compel serious reflection, and kids will not stop buying soda, candy, ice cream bars or chips.
HHS's Failure to Help Smokers Quit
Admissions about not having enough time to coordinate battle planning becomes painfully visible when reviewing the accuracy of quit smoking advice presented on the leading HHS quitting site SmokeFree.gov.
While inter-agency communication data from the new study is now five years old (2005), SmokeFree.gov evidences how little things have changed and the degree of continuing pharmaceutical influence over these eleven federal agencies. The right hand not knowing what the left was doing, defenseless, easy, and isolated pickings have allowed industry influence to transform government quitting sites such as SmokeFree.gov into little more than online drug stores.
 The #1 Internet quit smoking site, smokers and quitters exploring SmokeFree.gov are bombarded with 173 invitations to use "medication." Although cold turkey will again this year produce more ex-smokers than all other quitting methods combined, not a single Smokefree.gov web page encourages, defends, promotes or teaches successful cold turkey quitting.
The #1 Internet quit smoking site, smokers and quitters exploring SmokeFree.gov are bombarded with 173 invitations to use "medication." Although cold turkey will again this year produce more ex-smokers than all other quitting methods combined, not a single Smokefree.gov web page encourages, defends, promotes or teaches successful cold turkey quitting.
Pharmaceutical industry influence continues its stranglehold over Smokefree.gov's primary creator, the Tobacco Control Research Branch (TCRB) of the National Cancer Institute (NCI).
Interestingly, the primary author of this just released HHS inter-agency communication study, Scott J. Leischow, PhD, is also listed at SmokeFree.gov as a site developer and advisor. Dr. Leischow disclosed as part of a March 11, 2009 Journal of the American Medical Association article that he is a "paid speaker for Pfizer" (which sells Chantix) and a "consultant for Johnson & Johnson" (which sells replacement nicotine products including Nicorette).
SmokeFree.gov also lists Michael Cummings, PhD as a "notable" collaborator. A March 2009 journal article disclosed that Dr. Cummings has "received payment from Pfizer to speak to health professionals about their new stop-smoking medication, Chantix."
The NCI either remained silent or was not communicating with the Agency for Healthcare Research and Quality (AHRQ) when in 1999 AHRQ appointed a panel of experts having strong financial ties to the pharmaceutical industry and charged it with rewriting official U.S. quitting policy.
The panel published its recommendations in June 2000. One recommendation consumed all others. "There are numerous effective medications for tobacco dependence," the panel proclaimed, "and clinicians should encourage their use by all patients attempting to quit smoking."
With a single document, a single recommendation, the panel had effectively outlawed all government assistance of cold turkey quitting. Competition silenced, tens of thousands of federal, state and local health employees were instantly transformed into "medication" salesmen, guaranteeing the pharmaceutical industry billions in profits.
How has the National Cancer Institute reacted? Today, it continues to serve as the #1 driver of an Internet money train transporting smokers from SmokeFree.gov to neighborhood drug stores, where many will be new regular customers for years.
As the NCI is aware, and as President Obama can attest, replacement nicotine hooks a substantial percentage of quitters (up to 7% of quitters using nicotine gum). The ironic part is that while the NCI's primary mission is cancer prevention, it's fully aware that replacement nicotine elevates levels of the carcinogen NNN, promotes tumor growth and cell division via angiogenesis, inhibits chemotherapy effectiveness by preventing natural cell death (apoptosis), and accelerates the growth and spreading of cancer throughout the body.
Industry influence has so deeply infected all levels of HHS cessation thinking that there seems little hope of capping the well. How bad is it? During 2007 the NCI co-sponsored a 3 day industry sales conference where the Who's Who of pharmaceutical industry consultants openly advocated use of tobacco industry marketing tactics in order to sell even greater quantities of replacement nicotine.
Imagine the insanity of teaching alcoholics that pharmaceutically sold replacement alcohol is "medicine" and its use "therapy." Thanks to a lack of nicotine dependency recovery understanding and effective leadership within HHS, that's exactly where 37.6 million daily smokers now find themselves.
As noted by TCRB Chief Cathy L. Backinger, PhD, "tobacco use remains the country's leading cause of premature, preventable death - including an estimated one-third of all cancer deaths." Still, TCRB staff members have continued to push replacement nicotine having strong cancer promotion ties, even as it watched the medication era bring decline in the U.S. smoking rate to a standstill.
The question Dr. Backinger is hopefully asking herself is why Smokefree.gov continues to turn its back on the education and support needs of millions of cold turkey quitters. Are TCRB's cessation policy and quitting lessons responsible for an actual increase in smoking related cancers and disease? Does the National Cancer Institute share a degree of culpability in the cessation failures and deaths of thousands of smokers annually?
HHS Misrepresents "Your" Chances
Smokefree.gov's "Medications to Help You Quit" page states that "medicines can double your chances of quitting for good." Its "Quit Guide" again echoes that "medicines can double your chances of quitting for good." Its "Dispelling Myths about Nicotine Replacement Therapy" page continues the drum roll that, "NRT can double a smoker's chances of quitting smoking." And the chorus reaches crescendo inside the site's Clearing the Air quitting booklet which claims, "Studies show that these medications, compared with trying to quit without them, can double or triple your chances of quitting for good."
TCRB's double "your" chances campaign isn't limited to Smokefree.gov. Dr. Backinger presented a Powerpoint presentation in May 2007 claiming that, "pharmocotherapy can double the smoker's chance of quitting smoking." Why noteworthy? Because Dr. Backinger gave the presentation a year after a National Cancer Institute study found otherwise.
Far from doubling "your" chances, a 2006 NCI study found that those quitting without medications actually had slightly higher long-term success rates than those using medications. Yes, as horrible as this sounds, the NCI's Smokefree.gov web site evidences what may be the most deadly government health deception ever.

Pulitzer Prize winning journalist Kevin Helliker exposed the depth of pharmaceutical influence over HHS cessation policy in a 2007 front page Wall Street Journal article entitled, "Nicotine Fix - Behind Antismoking Policy, Influence of Drug Industry." The story shared unpublished data from a June 2006 NCI survey of 8,200 quitters. The study found that 14% quitting without medication were still not smoking after nine months, compared to only 12% among nicotine patch, gum and lozenge users.
Obviously, "no medication" quitters include more than just cold turkey quitters. But prior surveys suggest that all but about 2% are either cold turkey or smoking weaning/cut-down type quitters. Combined with recent research, it suggests that roughly 70% of no medication quitters are in fact cold turkey quitters. That same research shows that cold turkey success rates are nearly double those of smokers engaged in weaning/reduction schemes. If true, the NCI's lumping together of weaning with cold turkey under "no medication" heading masks an even greater cold turkey victory.

The National Cancer Institutes's real-world finding of medication failing to prevail over non-medication quitters is far from alone. Results of the world's largest smoking cessation survey were published in the September 2002 edition of the Journal of the American Medical Association. It concluded that, "NRT appears no longer effective in increasing long-term successful cessation in California smokers."

A 2006 Australian study followed the smoking patients of 1,000 family practice physicians. Not only did cold turkey success rates trounce medication quitters, the study found that cold turkey accounted for 1,942 of 2,207 former smokers, a whopping 88% of all success stories.
 Surveys from Canada and London also show medication failing to prevail over cold turkey. The UK's national smoking treatment program offers what is likely the highest quality local counseling and support cessation programs of any nation. There, those quitting without medication have a 67% higher one-year success rate than NRT quitters, and a 77% higher rate than Zyban quitters.
Surveys from Canada and London also show medication failing to prevail over cold turkey. The UK's national smoking treatment program offers what is likely the highest quality local counseling and support cessation programs of any nation. There, those quitting without medication have a 67% higher one-year success rate than NRT quitters, and a 77% higher rate than Zyban quitters.
Short term results (less than 6 months) are really rather meaningless when comparing cold turkey or "no medication" to "medication" success rates. When a study's medication use period lasts 3 months, at the 3 month mark the treated group is just beginning to attempt to live without chemical stimulation of brain dopamine pathways, while the placebo group's stimulation ended three months earlier. It's why such studies contrasting medication to no medication (placebo) inherently make medication appear 3 months better than reality.
While medications trounce placebo controls inside clinical trials, they fall flat on their face in real-world use. Why? While a number of factors play significant roles, the most profound is likely the fact that clinical trials pit medication quitters against quitters who joined seeking medication but didn't get it. It isn't until out in the real-world that medications are compelled to go head-to-head with real cold turkey quitters, quitters who fully expect to experience their withdrawal syndrome and successfully move beyond it.
The validity and scientific foundation of placebo-controlled cessation trials are rooted in the false assumption that these studies were blind, that participants were unable to quickly determine whether or not they had been randomly assigned to receive an inert placebo or the quitting product being tested (NRT, Zyban, Chantix or NicVax).
Researchers knowingly introduce expectations bias by dangling free quitting medicine in front of smokers to entice study participation. Today, nearly all researchers are aware that it's impossible to hide the onset of full-blown nicotine withdrawal from those with significant quitting histories, quitters expert at recognizing nicotine's absence. While the gold standard in most study areas, use of placebo controls in drug addiction studies has become a license to steal.
Experienced quitters randomly assigned to the placebo group should be expected to recognize withdrawal within 24 to 48 hours of stopping smoking. Placebo controlled smoking cessation trials do not measure a product's relative worth (efficacy) but the satisfaction or frustration of expectations.
How bad is it? When asked to guess their assignment, three to four times as many assigned to placebo correctly guess placebo as guess wrong. A recent study by the nicotine patch's co-inventor reported that "of 165 subjects receiving placebo patches, 27 believed they had received active patches, 112 believed they had not, and 26 were unsure."
Name any other study area where those assigned to the placebo group are punished with the onset of significant anxieties and made vastly worse than when they arrived. Name any other study area where the condition sought to be treated (chemical withdrawal) is non-existent until researchers command its onset ("ready, set, stop smoking nicotine").
It is normal to see 80% of the placebo group throw in the towel and relapse to smoking within the study's first week. If so, which group stands to benefit if the study has been designed to offer high quality weekly counseling or group support sessions during the entire 8 or 12 week treatment period?
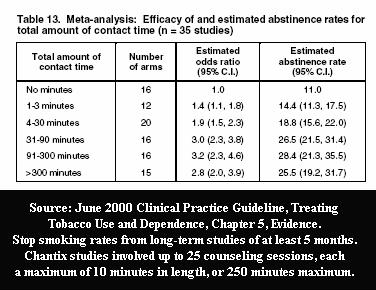
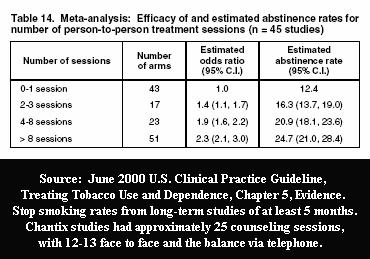
Official U.S. cessation policy acknowledges that counseling and support are "especially effective," easily doubling or tripling cessation rates based upon the amount of program contact time and number of sessions.
Pfizer's Chantix studies employed a record 25 counseling and support sessions. So how do we untangle Chantix's worth from counseling's? We can't. Amazingly, Pfizer's influence within the FDA was so great that the FDA approved Chantix (varenicline) without knowing its value as a stand-alone quitting aid.

"Population-based studies indicate that cold turkey cessation, not the use of NRT, is the most effective method for smoking cessation," wrote Michael Siegel, a physician and professor at Boston University School of Public Health. "It is time for a serious re-examination of both the effectiveness of nicotine replacement therapy and the role of NRT as part of a national strategy for the promotion of smoking cessation."
HHS Actually Undermines Successful Cold Turkey Quitting
Obviously, HHS and Secretary Sebelius realize that no visitor to Smokefree.gov will be attempting to quit while chewing, wearing or swallowing a placebo. But the site's assault upon cold turkey quitting goes far beyond misrepresenting that "your" chances if quitting cold turkey are identical to the clinical trial placebo quitter who wanted medicine but didn't get it. HHS goes out of its way to undermine and damage smoker/quitter beliefs and confidence in their own natural recovery instincts.
The Cold Turkey section of the Clearing the Air booklet featured at Smokefree.gov states, "For some smokers, 'going cold turkey' seems like the easiest way to quit: Just stop smoking and tell yourself you'll never light up again. This works for some smokers - usually those with the lowest level of nicotine dependence - but not many. Fewer than 5 percent of smokers can quit this way."
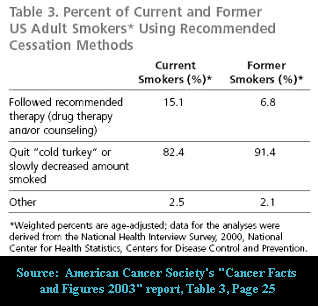 Ask yourself, is it fair to assert that this booklet suggests that only 1 in 20 smokers have the ability to quit cold turkey? If so, there's simply no polite way to say this, it's a lie. Nothing could be further from the truth. As the TCRB staff is fully aware, every quitting method survey ever conducted evidences that the vast majority of all successful long-term ex-smokers quit smoking cold turkey.
Ask yourself, is it fair to assert that this booklet suggests that only 1 in 20 smokers have the ability to quit cold turkey? If so, there's simply no polite way to say this, it's a lie. Nothing could be further from the truth. As the TCRB staff is fully aware, every quitting method survey ever conducted evidences that the vast majority of all successful long-term ex-smokers quit smoking cold turkey.
Recently an extended nicotine patch use study made worldwide headlines. If on the TCRB staff ask yourself this, how many study participants who wore the nicotine patch for up to 6 months were able to stop smoking for one full year? Answer: 2 of 282 patch users, a horrible one-year continuous cessation rate of 0.7%, a rate seven times worse than the often cited "unassisted" cold turkey one-year rate of 5%.
Not once on any Smokefree.gov web page does the TCRB "clear the air" and tell the truth about how most smokers really quit. Frankly, it cannot allow the truth to be known. Why? Because it would totally undermine the backbone of the entire site, its 173 invitations to buy and use "medication."
Not once on any Smokefree.gov page are smokers told medications one-year quitting rate. Why? Because when NRT is used without counseling or support its 6-month failure rate is in the neighborhood of 93%, and the industry continues to treat 1-year stand-alone rates as if top secret.
Instead, the site's Quitting Guide tells 100% of visitors that "quitting 'cold turkey' isn't your only choice. Talk to your doctor about other ways to quit ... They can suggest medicine to help with withdrawal."
Another Smokefree.gov tactic that undermines successful non-medication quitting is telling all arriving smokers they should wait to quit, that "your chances will be better if you get ready first," that "quitting works best when you're prepared," that you should "set a date" and "talk to your doctor" about "medicine."
This "Preparing to Quit" advice is totally contrary to two recent studies which found that unplanned quitting attempts are twice as likely to succeed as planned ones. A 2006 UK study taught the TCRB that "among respondents who had made a quit attempt between six months and five years previously the odds of success were 2.6 times higher in unplanned attempts than in planned attempts." This finding was duplicated in a 2009 study (by acknowledged GlaxoSmithKline consultants, the maker of Nicorette gum), which found that "the odds of a 'spontaneous' quit attempt lasting for 6 months or longer were twice that of preplanned attempts."
Teaching nicotine addicts to wait and choose "a special day" such as "your birthday or wedding anniversary, New Year's Day, Independence Day, World No Tobacco Day (May 31) or The Great American Smokeout (the third Thursday of each November)" doubles their likelihood of failure.
Clearly, current medication use policies of both the NCI and CDC are well served by creating time to allow for its purchase. But telling a nicotine addict who is contemplating cessation to delay quitting both creates time for postponement excuses to arise ("things are just too stressful right now"), or for the gradual building and escalation of resolve destroying fears and anxieties, as they anticipate quitting day growing near.
The TCRB statement that "quitting works best when you prepare" is false. The question all HHS staffers need to ponder is why this advice has been allowed to remain for more than a year after the second study, and how many successful quitting attempts the site's delay advice has cost.
Related SmokeFree.gov anxiety generating advice is that "Instead of smoking" ... "Think about something else." A July 2010 study reports that attempts at thought suppression actually increase unwanted thoughts, resulting in significantly more stress than when advised to think about and focus upon them.
From advice to avoid confronting and extinguishing subconscious cue conditioning, to recommendations that quitters make major life style changes or adopt replacement crutches, sadly, the site is filled with similar instances where quit destructive advice is contrary to both common sense and study evidence. What's heartbreaking is that no one within HHS or the NCI seems to care.
HHS Hides Most Important Cold Turkey Lessons
While Smokefree.gov devotes 15 pages to teaching proper selection and use of medications, not a single page teaches corresponding concerns or critical lessons unique to successful abrupt nicotine cessation.
For example, a critical cold turkey lesson is that nicotine is no longer acting as the quitter's spoon, that they need to eat breakfast, lunch and dinner or expect to suffer the consequences. Nicotine stimulates the body's fight or flight response, feeding smokers instant energy via release of stored fats and sugars. This allows smokers to develop a habit of skipping breakfast and even lunch without experiencing a host of low blood sugar symptoms that include cravings, anxiety, shakiness, confusion or difficulty concentrating, sweating, nervousness and weakness.
Cold turkey quitters benefit by knowing the importance of keeping blood sugar levels as stable as possible during early recovery, of eating healthy foods little and often, of not skipping meals. Unless their diet or health prohibits it, they benefit by knowing the value of natural fruit juices prior to peak withdrawal (day 3), in helping stabilize blood sugars and diminish needless symptoms. Acidic fruit juices also speed renal elimination of the alkaloid nicotine from the bloodstream, allowing the possibility of brain receptor re-sensitization and down-regulation a bit sooner.
Clearly, this lesson is unnecessary for quitters using replacement nicotine. In fact, Smokefree.gov teaches NRT quitters the exact opposite, that they need to "wait a half hour after using the gum, lozenge, or inhaler before you eat or drink anything acidic. Acidic foods and drinks can keep nicotine gum and inhalers from working. Acidic foods and drinks include tomato sauce, tomatoes, oranges, lemons, grapefruit, coffee, soda, orange juice, and grapefruit juice."
So, why is there no corresponding page teaching cold turkey quitters the value of acidic fruit juices in stabilizing blood sugars and accelerating nicotine elimination? Examples of additional missing cold turkey lessons include normal nicotine elimination rates, when peak withdrawal is achieved, how nicotine's absence doubles blood serum caffeine levels, the importance of being extremely careful with alcohol early on, cessation time distortion and crave episode duration.
But the most glaring Smokefree.gov absence is the "Law of Addiction," that "Administration of a drug to an addict will cause re-establishment of chemical dependence upon the addictive substance." HHS keeps hidden the science showing that just one puff of nicotine and up to 50% of the smoker's nicotinic-type acetylcholine receptors will become occupied by nicotine. While the majority of smokers walk away from relapse thinking that they succeeded in smoking just one, they soon find their brain begging for more.
Which of the following two statements are true? "Research shows that if you have even one cigarette after quitting, there is a 90% chance that you will return to regular smoking" or "Don't be discouraged if you slip up and smoke one or two cigarettes. It's not a lost cause. One cigarette is better than an entire pack"?
Shockingly, these conflicting lessons are found in different places on Smokefree.gov. The "90%" relapse quote is contained in a not so easy to locate brochure by Forever Free entitled "What if You Have a Cigarette." The "not a lost cause" contention is a featured segment in the site's Quit Guide. It's as if the TCRB is unaware of the relapse research of Brandon and Boreland.
Imagine advising an alcoholic not to get discouraged if you have a drink or two, or a heroin addict not to worry about shooting-up once or twice, that it's not a lost cause. Such advice may not be damaging to replacement nicotine users who have yet to stop using, but to a cold turkey quitter, who likely expended substantial resolve in breaking free from nicotine, it's an invitation to fail.
Pretend that you're a cold turkey quitter on day 4 and now residing inside a nicotine-free body, yet fixated on the thought of smoking just one. Imagine visiting a government site that teaches that smoking one or two cigarettes isn't a lost cause. How many lives is such advice costing? Sadly, HHS's handling of the most critical recovery lesson of all is so weak that it actually invites the recovering addict's mind to smoke and fail.
Teaching that lapse "is not a lost cause" defies nicotine dependency physiology. Withdrawal isn't a matter of choice or controlling discouragement but about brain function. Teaching nicotine addicts that they should be able to endure successive periods of the most challenging portion of recovery (the first three days of nicotine detox) is likely to result in creation of their greatest cessation defeat ever, causing fear, delay and postponement of future attempts.
Smokers need to be taught the truth, that just one puff of nicotine and relapse is all but assured. Instead, the TCRB sugar-coats and hides defeat behind the harmless word "slip," while sacrificing the greater good. Although full relapse following a "slip" is not 100% guaranteed, it's so close that the massive relapse prevention benefits flowing from having all quitters see, treat and act as though lapse equals relapse vastly exceeds the benefits of asking them to attempt to defy nicotine brain physiology.
Instead of teaching the secret to success, HHS teaches that it takes the average quitter multiple attempts before learning what it takes to quit and stay quit? Why not instead teach that if you take a puff you lose? Why not teach that all can succeed on their very first try, that there is only one rule that if followed provides a 100% guarantee of doing so ... no nicotine today!
Besides depriving cold turkey quitters of the most important quitting lesson of all, not a single Smokefree.gov page attempts to instill confidence in cold turkey quitting. Instead they attempt to get them to purchase "medicines," products that have already failed the vast majority of daily smokers.
Nearly three decades of quitting meds marketing has bombarded cold turkey quitters with the message that their odds of failure are double, that you have to be a super hero to succeed without meds. It's really rather amazing that most quitters continue to trust their own natural recovery instincts over the experts. What sense does it make to deprive such determination the encouragement, education and support needed to savor success?
Quitting cold turkey does not mean quitting in ignorance or darkness or without quality support. Nicotine is only a chemical with an IQ of zero. It cannot think, plan, plot or conspire, and is not some demon that dwells within. Although quitters will never be stronger than nicotine, they don't need to be. Their greatest weapon has always been their vastly superior intelligence but only if put to work.
What learning takes place by slapping on a patch, swallowing a pill, sucking a lozenge or chewing nicotine gum? HHS's fear of creating web pages that motivate, encourage, teach and support America's most productive quitting method is that visibly doing so will result in fewer quitters using "medication."
In other words, HHS intentionally ignores the cessation needs of the vast majority of quitters in order to motivate use of products, which according to its own surveys are less effective in real-world use than quitting without them.
HHS's objective should be to make every visiting nicotine addict more dependency recovery intelligent than their addiction is strong.
This new agency interactions study found that inter-agency communication failures may be compromising the mission. While the authors were gentle, kind and stopped short of casting blame, there's abundant evidence that failure to communicate and coordinate in both protecthttp://youtu.be/g8XvSiHmlQ8ing youth and assisting quitters is costing thousands their lives.
Although the study doesn't say it, if the primary purpose of the HHS tobacco control network is to provide entrenched health bureaucrats with job security then Congress needs to pull the funding plug. If HHS Secretary Kathleen Sebelius is serious about battling this nation's biggest killer, it cannot begin until she both addresses HHS's tobacco health leadership disaster and puts an end to allowing quitting product salesmen to author war plans.

{kind=link}
{kind=link}
{kind=link}
{kind=link}