
Smokefree.gov really Buymeds.now
NOTE: The Smokefree.gov website underwent a massive makeover on or about August 1, 2013. Using the Internet Archive (Wayback Machine), links on this page continue to share how SmokeFree.gov appeared when this 2010 article was written. An aside, the August 2013 makeover continues to grossly exaggerate the real-world worth of horribly ineffective approved quitting products.
For example, U.S. health officials continue to ignore all long-term population level findings in falsely suggesting that for the past 30 years Nicorette nicotine gum has doubled quitter success rates. Nothing could be further from the truth. According to a July 2013 Gallup poll, only 1 in 100 successful U.S. ex-smokers credit nicotine gum for their success. As I ask in a November 2013 BMJ letter, "How much closer to consumer fraud can approved products get?"

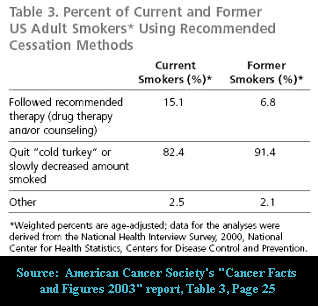
The #1 government quit smoking site is Smokefree.gov. Once there, smokers and quitters are bombarded with 173 invitations to use "medication" or "medicine." Cold turkey will again this year produce more ex-smokers than all other quitting methods combined, yet not a single Smokefree.gov webpage encourages, defends, promotes or teaches successful cold turkey quitting.
Pharmaceutical industry influence, too thick to cut with a chainsaw, continues its stranglehold over Smokefree.gov's creator, the Tobacco Control Research Branch (TCRB) of the National Cancer Institute (NCI). The NCI remained silent when in June 2000 a panel of experts with strong financial ties to the pharmaceutical industry was allowed to write official U.S. quitting policy. "There are numerous effective medications for tobacco dependence," the panel proclaimed, "and clinicians should encourage their use by all patients attempting to quit smoking."
Keyboard strokes of genius, the expert panel effectively outlawed all government assistance of cold turkey quitting. Competition silenced, tens of thousands of federal, state and local health employees were instantly transformed into "medication" salesmen, guaranteeing the pharmaceutical industry billions.
How has the National Cancer Institute reacted? Today, it's the #1 driver of an Internet money train between smokers filled with carcinogen time-bombs and industry coffers filled with replacement nicotine receipts. As the NCI is aware, replacement nicotine hooks a substantial percentage of quitters (up to 7% of nicotine gum users), elevates levels of the carcinogen NNN, promotes tumor growth and cell division via angiogenesis, inhibits chemotherapy effectiveness by preventing natural cell death (apoptosis), and accelerates the growth and spreading of cancer throughout the body.
Industry influence has so deeply infected all levels of government cessation thinking that there's little hope of reversing course. How bad is it? The NCI co-sponsored a 3 day industry sales conference where the Who's Who of pharmaceutical industry consultants openly advocated use of tobacco industry marketing tactics, in order to sell even greater quantities of replacement nicotine.
Imagine the chaos, cessation mess and lessons not learned if alcoholics were taught that pharmaceutically sold replacement alcohol was "medicine" and its use "therapy." Thanks to a lack of nicotine dependency recovery understanding and effective leadership within the National Cancer Institute and Centers for Disease Control, that's exactly where 37.6 million daily smokers now find themselves.
As noted by TCRB Chief Cathy L. Backinger, PhD, "tobacco use remains the country's leading cause of premature, preventable death - including an estimated one-third of all cancer deaths." Still, TCRB staff members have continued to push replacement nicotine having strong cancer promotion ties, even as it watched the medication era bring decline in the U.S. smoking rate to a standstill.
The question Dr. Backinger is hopefully asking herself is why Smokefree.gov continues to turn its back on the education and support needs of millions of cold turkey quitters? Are TCRB's cessation policy and quitting lessons responsible for an actual increase in smoking related cancers and disease? Does the National Cancer Institute share a degree of culpability in the cessation failure and deaths of thousands of smokers?
National Cancer Institute Misrepresents "Your" Chances
Smokefree.gov's "Medications to Help You Quit" page states that "medicines can double your chances of quitting for good." Its "Quit Guide" again echoes that "medicines can double your chances of quitting for good." Its "Dispelling Myths about Nicotine Replacement Therapy" page continues the drum roll that, "NRT can double a smoker's chances of quitting smoking." And the chorus reaches crescendo inside the site's Clearing the Air quitting booklet which claims, "Studies show that these medications, compared with trying to quit without them, can double or triple your chances of quitting for good."
TCRB's double "your" chances campaign isn't limited to Smokefree.gov. Dr. Backinger presented a Powerpoint presentation in May 2007 claiming that, "pharmocotherapy can double the smoker's chance of quitting smoking." Why noteworthy? Because Dr. Backinger gave the presentation a year after a National Cancer Institute study found otherwise.
Far from doubling "your" chances, a 2006 NCI study found that those quitting without medications actually had slightly higher long-term success rates than those using medications. Yes, as horrible as this sounds, the NCI's Smokefree.gov website evidences what may be the most deadly government health deception ever.

Pulitzer Prize winning journalist Kevin Helliker exposed the depth of pharmaceutical influence over NCI cessation policy in a 2007 front page Wall Street Journal article entitled, "Nicotine Fix - Behind Antismoking Policy, Influence of Drug Industry." The story shared unpublished data from a June 2006 NCI survey of 8,200 quitters. The study found that 14% quitting without medication were still not smoking after nine months, compared to only 12% among nicotine patch, gum and lozenge users.
Obviously, "no medication" quitters include more than just cold turkey quitters, but prior surveys suggest that all but about 2% are either cold turkey quitters or smoking reduction/cut-down type quitters. Combined with recent research, it suggests that roughly 70% of no medication quitters are cold turkey quitters. That same research also shows that cold turkey success rates are nearly double those of smokers engaged in weaning/reduction schemes. If true, the NCI's lumping together of less effective "no medication" quitters masks a greater cold turkey victory.

The National Cancer Institute's real-world finding of medication failing to prevail over non-medication quitters is far from alone. Results of the world's largest smoking cessation survey were published in the September 2002 edition of the Journal of the American Medical Association. It concluded that, "NRT appears no longer effective in increasing long-term successful cessation in California smokers."

A 2006 Australian study followed the smoking patients of 1,000 family practice physicians. Not only did cold turkey success rates trounce medication quitters, the study found that cold turkey accounted for 1,942 of 2,207 former smokers, a whopping 88% of all success stories.
 Surveys from Canada and London also show medication failing to prevail over cold turkey. The UK's national smoking treatment program offers what is likely the highest quality local counseling and support cessation programs of any nation. There, those quitting without medication have a 67% higher one-year success rate than NRT quitters, and a 77% higher rate than Zyban quitters.
Surveys from Canada and London also show medication failing to prevail over cold turkey. The UK's national smoking treatment program offers what is likely the highest quality local counseling and support cessation programs of any nation. There, those quitting without medication have a 67% higher one-year success rate than NRT quitters, and a 77% higher rate than Zyban quitters.
Short term results (less than 6 months) are really rather meaningless when comparing cold turkey or "no medication" to "medication" success rates. When a study's medication use period lasts 3 months, at the 3 month mark the treated group is just beginning to attempt to live without chemical stimulation of their brain dopamine pathways, while the placebo group's stimulation ended three months earlier. It's why such studies contrasting medication to no medication (placebo) inherently make medication appear up to 3 months better than reality.
While medications trounce placebo controls inside clinical trials, they fall flat on their face in real-world use. Why? While a number of factors play significant roles, the most profound is likely the fact that clinical trials pit medication quitters against quitters who joined seeking medication but didn't get it. It isn't until out in the real-world that medications are compelled to go head-to-head with real cold turkey quitters, quitters who fully expect to experience their withdrawal syndrome and successfully move beyond it.
The validity and scientific foundation of placebo-controlled cessation trials are rooted in the false assumption that these studies were blind, that participants were unable to determine whether or not they had been randomly assigned to receive an inert placebo or the quitting product being tested (NRT, Zyban or Chantix).
Researchers knowingly introduce expectations bias by dangling free quitting medicine in front of smokers to entice study participation. Today, nearly all researchers are aware that it's impossible to hide the onset of full-blown nicotine withdrawal from smokers with lengthy quitting histories, quitters expert at recognizing nicotine's absence. While the gold standard in most study areas, use of placebo controls in drug addiction studies is license to steal.
Experienced quitters randomly assigned to the placebo group should be expected to recognize withdrawal within 24 to 48 hours of stopping smoking. Placebo controlled smoking cessation trials do not measure a product's relative worth (efficacy) but the satisfaction and frustration of expectations.
How bad is it? When asked to guess their assignment, three to four times as many assigned to placebo correctly guess placebo as guess wrong. A recent study by the nicotine patch's co-inventor reported that "of 165 subjects receiving placebo patches, 27 believed they had received active patches, 112 believed they had not, and 26 were unsure." Yes, four times as many correctly identified their assignment as could not.
Name any other study area where those assigned to the placebo group are punished with the onset of significant anxieties and made vastly worse than when they arrived. Name any other study area where the condition sought to be treated (chemical withdrawal) is nonexistent until researchers command its onset ("ready, set, stop smoking nicotine").
It is normal to see 80% of the placebo group throw in the towel and relapse to smoking within the study's first week. If true, which group stands to benefit if the study has been designed to offer once a week sessions of quality counseling and/or support?
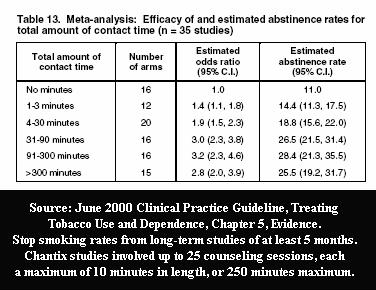
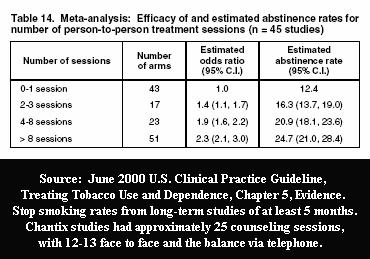
Official U.S. cessation policy acknowledges that counseling and support are "especially effective," easily doubling or tripling cessation rates based upon the amount of program contact time and number of sessions. Pfizer's Chantix studies employed a record 25 counseling and support sessions. So how do we untangle Chantix's worth from counseling's? We can't. Amazingly, Pfizer's influence within the FDA is so great that the FDA approved Chantix (varenicline) without knowing its value as a stand-alone quitting aid.
"Population-based studies indicate that cold turkey cessation, not the use of NRT, is the most effective method for smoking cessation," wrote Michael Siegel, a physician and professor at Boston University School of Public Health, "It is time for a serious re-examination of both the effectiveness of nicotine replacement therapy and the role of NRT as part of a national strategy for the promotion of smoking cessation."
National Cancer Institute Undermines Successful Cold Turkey Quitting
Obviously, TCRB staff members realize that no visitor to Smokefree.gov will be attempting to quit while chewing, wearing or swallowing a placebo. But their assault upon cold turkey quitting goes far beyond misrepresenting that "your" chances if quitting cold turkey are identical to the clinical trial placebo quitter who wanted medicine but didn't get it. The TCRB goes out of its way to undermine and damage smoker/quitter beliefs and confidence in their own natural quitting instincts.
The Cold Turkey section of the Clearing the Air booklet featured at Smokefree.gov states, "For some smokers, 'going cold turkey' seems like the easiest way to quit: Just stop smoking and tell yourself you'll never light up again. This works for some smokers - usually those with the lowest level of nicotine dependence - but not many. Fewer than 5 percent of smokers can quit this way."
 Ask yourself, is it fair to assert that this booklet suggests that only 1 in 20 smokers have the ability to quit cold
turkey? If so, there's simply no polite way to say this, it's a lie. Nothing could be further from the truth. As the TCRB staff is fully aware, every quitting method survey ever conducted evidences that the vast majority of all successful long-term ex-smokers quit smoking cold turkey.
Ask yourself, is it fair to assert that this booklet suggests that only 1 in 20 smokers have the ability to quit cold
turkey? If so, there's simply no polite way to say this, it's a lie. Nothing could be further from the truth. As the TCRB staff is fully aware, every quitting method survey ever conducted evidences that the vast majority of all successful long-term ex-smokers quit smoking cold turkey.
Last month, the extended nicotine patch use study made worldwide headlines. If on the TCRB staff ask yourself this, how many study participants who wore the nicotine patch for up to 6 months were able to stop smoking for one full year? Answer: 2 of 282 patch users, a horrible one-year continuous cessation rate of 0.7%, a rate seven times worse than the often cited "unassisted" cold turkey rate of 5%.
Not once on any Smokefree.gov web page does the TCRB "clear the air" and tell the truth about how most smokers really quit. Frankly, it cannot allow the truth to be known. Why? Because it would totally undermine the backbone of the entire site, its 173 invitations to buy and use "medication" or "medicine."
Not once on any Smokefree.gov page are smokers told medications one-year quitting rate. Why? Because when NRT is used without counseling or support its 6-month failure rate is in the neighborhood of 93%, and the industry continues to treat 1-year stand-alone rates as if top secret.
Instead, the site's Quitting Guide tells 100% of visitors that "quitting 'cold turkey' isn't your only choice. Talk to your doctor about other ways to quit ... They can suggest medicine to help with withdrawal."
Another Smokefree.gov tactic that undermines successful cold turkey quitting is telling all arriving smokers they should wait to quit, that "your chances will be better if you get ready first," that "quitting works best when you're prepare," that you should "set a date" and "talk to your doctor" about "medicine."
This "Preparing to Quit" advice is contrary to two recent studies which found that unplanned quitting attempts are twice as likely to succeed as planned attempts. A 2006 UK study taught the TCRB that "among respondents who had made a quit attempt between six months and five years previously the odds of success were 2.6 times higher in unplanned attempts than in planned attempts." This finding was duplicated in a 2009 study (by acknowledged GlaxoSmithKline consultants, the maker of Nicorette gum), which found that "the odds of a 'spontaneous' quit attempt lasting for 6 months or longer were twice that of preplanned attempts."
Teaching nicotine addicts to wait and choose "a special day" such as "your birthday or wedding anniversary, New Year's Day, Independence Day, World No Tobacco Day (May 31) or The Great American Smokeout (the third Thursday of each November)" doubles their likelihood of failure.
Clearly, current medication use policies of both the National Cancer Institute and Centers for Disease Control are well served by creating time to allow for its purchase. But telling a nicotine addict who is contemplating cessation to delay quitting both creates time for postponement excuses to arise ("things are just too stressful right now"), or for the gradual building and escalation of resolve destroying fears and anxieties, as they anticipate quitting day growing near.
The TCRB statement that "quitting works best when you prepare" is false. The questions TCRB staffers need to ponder are, why this advice has been allowed to remain, and how many successful quitting attempts the site's delay advice has cost?
National Cancer Institute Hides Cold Turkey Lessons
While Smokefree.gov devotes 15 pages to teaching proper selection and use of medications, not a single page teaches corresponding concerns or critical lessons unique to successful abrupt nicotine cessation quitting.
For example, a critical cold turkey lesson is that nicotine is no longer acting as the quitter's spoon, that they need to eat breakfast, lunch and dinner or expect to suffer the consequences. Nicotine stimulates the body's fight or flight response, feeding smokers instant energy via release of stored fats and sugars. This allows smokers to develop a habit of skipping breakfast and even lunch without experiencing a host of low blood sugar symptoms that include cravings, anxiety, shakiness, confusion or difficulty concentrating, sweating, nervousness and weakness.
Cold turkey quitters benefit by knowing the importance of keeping blood sugar levels as stable as possible during early recovery, of eating healthy foods little and often, of not skipping meals. Unless their diet or health prohibits it, they benefit by knowing the value of natural fruit juices prior to peak withdrawal (day 3), in helping stabilize blood sugars and diminish needless symptoms. Acidic fruit juices also speed renal elimination of the alkaloid nicotine from the bloodstream, allowing the possibility of brain receptor re-sensitization and down-regulation a bit sooner.
Clearly, this lesson is unnecessary for quitters using replacement nicotine. In fact, Smokefree.gov teaches NRT quitters the exact opposite, that they need to "wait a half hour after using the gum, lozenge, or inhaler before you eat or drink anything acidic. Acidic foods and drinks can keep nicotine gum and inhalers from working. Acidic foods and drinks include tomato sauce, tomatoes, oranges, lemons, grapefruit, coffee, soda, orange juice, and grapefruit juice."
So, why is there no corresponding page teaching cold turkey quitters the value of acidic fruit juices in stabilizing blood sugars and accelerating nicotine elimination? Examples of additional missing cold turkey lessons include normal nicotine elimination rates, when peak withdrawal is achieved, how nicotine's absence doubles blood serum caffeine levels, the importance of being extremely careful with alcohol early on, cessation time distortion and crave episode duration.
But the most glaring Smokefree.gov absence is the "Law of Addiction," that "Administration of a drug to an addict will cause re-establishment of chemical dependence upon the addictive substance." TCRB keeps hidden the science showing that just one puff of nicotine and up to 50% of the smoker's nicotinic-type acetylcholine receptors will become occupied by nicotine. While the majority of smokers walk away from relapse thinking that they succeeded in smoking just one, their brain is soon begging for more.
Which of the following two statements are true? "Research shows that if you have even one cigarette after quitting, there is a 90% chance that you will return to regular smoking" or "Don't be discouraged if you slip up and smoke one or two cigarettes. It's not a lost cause. One cigarette is better than an entire pack"?
Shockingly, these conflicting lessons are found in different places on Smokefree.gov. The "90%" relapse quote is contained in a not so easy to locate brochure by Forever Free entitled "What if You Have a Cigarette." The "not a lost cause" contention is a featured segment in the site's Quit Guide. It's as if the TCRB is unaware of the relapse research of Brandon and Boreland.
Imagine advising an alcoholic not to get discouraged if you have a drink or two, or a heroin addict not to worry about shooting-up once or twice, that it's not a lost cause. Such advice may not be damaging to replacement nicotine users who have yet to stop using, but to a cold turkey quitter, who likely expended substantial resolve in breaking free from nicotine, it's an invitation to fail.
Pretend that you're a cold turkey quitter on day 4, now residing inside a nicotine-free body, yet fixated on the thought of smoking just one. Imagine visiting a government quitting site that teaches you that smoking one or two cigarettes isn't a lost cause, when the site's creators know that roughly 90% who smoke just one cigarette experience full relapse. How many lives could such advice cost? Sadly, the Institute's handling of the most critical recovery lesson of all is so weak that it actually invites the recovering addict's mind to smoke and fail.
Teaching that lapse "is not a lost cause" defies nicotine dependency physiology. Withdrawal isn't a matter of choice or controlling discouragement but about brain function. Teaching nicotine addicts that they should be able to endure successive periods of the most challenging portion of recovery (withdrawal) is likely to result in creation of their greatest cessation defeat ever, causing delay and postponement of future attempts.
Smokers need to be taught the truth, that just one puff of nicotine and relapse is all but assured. Instead, the TCRB sugar-coats and hides defeat behind the harmless word "slip," while sacrificing the greater good. Although full relapse following a "slip" is not 100% guaranteed, it's so close that the massive relapse prevention benefits flowing from having all quitters treat, see and act as though lapse equals relapse vastly exceeds the benefits of asking them to defy nicotine brain physiology.
Why hide the secret to success by teaching that it takes the average quitter a specified number of attempts before learning what it takes to quit and stay quit? Why not teach that if you take a puff you lose? Why not teach that all can succeed on their very first try, that there is only one rule that if followed provides a 100% guarantee of doing so ... no nicotine today!
Besides depriving cold turkey quitters of the most important quitting lesson of all, not a single Smokefree.gov page attempts to instill confidence in cold turkey quitting. Instead it attempts to get them to use "medicines" that have already failed the vast majority of daily smokers.
Nearly three decades of quitting meds marketing has bombarded cold turkey quitters with the message that their odds of failure are double, that you have to be a super hero to succeed without meds. It's really rather amazing that most quitters continue to trust their own natural recovery instincts over the experts." What sense does it make to deprive such determination the encouragement, education and support needed to allow instinct to savor success?
Quitting cold turkey does not mean quitting in ignorance or darkness or without quality support. Nicotine is only a chemical with an IQ of zero. It cannot think, plan, plot or conspire, and is not some demon that dwells within. Although quitters will never be stronger than nicotine, they don't need to be. A quitter's greatest weapon is their vastly superior intelligence but only if put to work.
What learning takes place by slapping on a patch, swallowing a pill, sucking a lozenge or chewing nicotine gum? The TCRB's fear of creating web pages that motivate, encourage, teach and support America's most productive quitting method is that visibly doing so will result in fewer quitters using "medication." In other words, the TCRB intentionally ignores the cessation needs of the vast majority of quitters in order to motivate use of products, which according to the Institute's own survey are less effective in real-world use than quitting without them.
The NCI's objective should be to make every visiting nicotine addict more dependency recovery intelligent than their addiction is strong. Instead, it compels cold turkey quitters to view "medication" links on 49 web pages, links telling them that they're going about it all wrong. While I would remove all medication links, at least by putting cold turkey links beside medication links, quitters would be presented an option. As now presented, there is none.
National Cancer Institute Endangers Fetal Development
Smokefree.gov's presentation of replacement nicotine to pregnant women is reckless. The NCI knows that nicotine is a neurobehavioral fetal teratogen that damages normal brain development and is believed responsible for attention deficit hyperactivity disorder, learning disabilities and conduct disorders. It also knows that the nicotine patch overwhelms placenta filtering, which can result in fetal brain nicotine levels three times higher than seen in the mother's blood serum. It also knows that replacement nicotine has not shown efficacy or effectiveness as a stand-alone pregnancy quitting aid.
Worst of all, Smokefree.gov implying that replacement nicotine may be safely used during pregnancy likely causes thousands of expectant women, who otherwise could have quit altogether, to instead expose the fetus to months of nicotine. Picture that nicotine attempting to stimulate fetal brain receptors before the associated neuron is developed and functional. According to toxicologists, it's how nicotine destroys normal fetal brain development trajectories.
Each of Smokefree.gov's NRT pages draws the pregnant smoker's attention to a "Special Precautions" heading entitled "Pregnancy/breastfeeding." There they are told that, "Smokers who are pregnant or breastfeeding should try to quit first without using [replacement] nicotine. [Replacement] nicotine should be used during pregnancy only if the associated benefits outweigh the associated risks."
How many drawn to each NRT page's pregnancy heading will leave believing that government health officials say it's safe to use replacement nicotine during pregnancy?
While the final sentence of the topic immediately above the pregnancy heading states, "If you are pregnant, breastfeeding, or have a severe medical problem, talk with your doctor before starting any new medication," why wasn't this statement included under the "Pregnancy/breastfeeding" heading? Nicotine is a super toxin, the tobacco plant's natural insecticide. It has no business inside the fetus. Contrary to cigarette pack warnings, it is no longer a question of whether or not nicotine will damage fetal development but how profound the damage will be.
Additional Disturbing Smokefree.gov Pages
Before being critical of non-science-based lessons taught on most Smokefree.gov web pages, I note that the site's Depression Basics page is outstanding. This high quality depression teaching tool is invaluable in light of the FDA having linked Chantix to depressed mood and suicide. I'd only change one thing: there's no need to pollute the page with links to quitting medications.
Varenicline Fact Sheet - The NCI and the TCRB are fully aware that on July 1, 2009, that the FDA assigned Chantix the highest risk warning category of all, requiring a black boxed warning associated with "serious mental health events including changes in behavior, depressed mood, hostility, and suicidal thoughts." The FDA has received more than a thousand reports of serious adverse events while using Chantix, 101 during the 3rd quarter of 2009, and wrongful death lawsuits are being filed alleging that varenicline was responsible for causing suicide.
Smokefree.gov's Chantix web page fails to include the highlighted portion of the FDA's July 1, 2009 Public Health Advisory or a link to the advisory. Also absent is a link to an FDA video clip detailing serious adverse events linked to Chantix. Instead, the TCRB substitutes the word "rare" for "serious" in describing key FDA adverse event findings.
More disturbing, the TCRB provides a link to the FDA's home page, making it highly unlikely readers will successfully locate the FDA's latest warning, advisory or video clip. Why no direct links to FDA warnings? It's as if the TCRB allowed Pfizer, Chantix's maker, to write this page.
Bupropion Fact Sheet - This page makes no mention of the fact that on July 1, 2009, the FDA assigned bupropion, marketed as Zyban or Wellbutrin, the highest risk warning category of all, requiring a black boxed warning. It fails to tell readers that the FDA has linked bupropion to "serious mental health events including changes in behavior, depressed mood, hostility, and suicidal thoughts" and fails to provide a link to either the FDA's boxed warning announcement or its latest Public Health Advisory.
Nicotine Gum Fact Sheet - This page fails to tell readers that up to 7% of nicotine gum quitters become persistent long term users of at least 6 months. Recall that the NCI's 2006 survey found that 14% of nicotine gum quitters were still not smoking at 9 months. In that numerous studies have linked nicotine to cancer promotion (search: nicotine + cancer) and long-term gum users report a host of health concerns, does informed consent demand that the NCI share nicotine gum dependency findings when up to 50% of successful gum quitters find themselves hooked on the cure?
Why quitting is so hard - This page fails to answer the title's question, why quitting is so hard. It's hard because those teaching that nicotine is medicine have so muddied natural learning that it has become harder than ever to self-discover the Law of Addiction via the school of hard-quitting-knocks.
Instead of teaching the power of a puff to destroy a quitting effort, the page pleads ignorance of the ultimate lesson needed to succeed. It tells readers that, "It takes time to break free from nicotine addiction. It may take more than one try to quit for good." "It may take several tries. But you learn something each time you try."
"Several tries?" Why suggest defeat? Why invite relapse? Why not instead teach the one lesson that if mastered guarantees success to all? There was always only one rule ... no nicotine today?
The page also fuels junkie thinking and relapse by teaching that, "You enjoy holding cigarettes and puffing on them. You may smoke when you are stressed, bored, or angry."
Why feed nicotine addicts false use rationalizations? Smokers don't smoke because they enjoy it, but because they don't enjoy what happens when they don't smoke. They don't hold or puff on cigarettes because they like to, they do so because they must, because they are true drug addicts in every sense, because their brain has been rewired to function on nicotine, because every two hours their body's nicotine reserves decline by half.
This page's smoking stress relief lesson is also contrary to the science-base. The TCRB fails to teach smokers that acid generating events such as stress, alcohol use and vitamin C accelerates renal elimination of the alkaloid nicotine from the bloodstream. Stressful events accelerate the need for replenishment, leaving the stressed smoker on the brink of withdrawal. They cannot turn their attention to the underlying stressful event (example: a flat tire) until their sagging nicotine reserves have been replenished.
More nicotine does not relieve stress but only its own absence. Smokers effectively add the onset of early withdrawal to stressful events. One of the simple joys often experienced during recovery is a surprising sense of calm during crisis.
Additionally, the page teaches that, "It takes willpower and strength to beat your addiction to nicotine." Dreams, desire and understanding, not strength or willpower, are the wind beneath the successful quitter's wings. Try using strength or willpower to stop inhaled nicotine from causing a brain dopamine explosion ten seconds later. Suggesting to smokers that they can become stronger than their addiction, or will it into submission, is a recipe for lifetime relapse.
Which is it? Near the top of the page smokers are taught that the secret to quitting is that "you learn something each time you try." Near the bottom they're taught that "willpower and strength" are key.
Quitters benefit by developing respect for the power of nicotine to alter brain receptor sensitivities and numbers, and hijack priorities. Teaching that strength and willpower are key can needlessly delay cessation until the quitter feels adequate reserves of both, until they feel stronger than their addiction. Why not teach them the truth. A simple desire to be free and respect for the Law of Addiction is all that's needed to experience lasting freedom.
Putting a Stop to Smoky Thinking - This page teaches smokers that, "It's normal to make some mistakes" and smoke cigarettes. Imagine teaching recovering alcoholics that, "it's normal to make a mistake and have a drink." This lesson shows a lack of understanding of chemical dependency and sets the stage for relapse and defeat.
The TCRB must end its role as relapse facilitator and start teaching smokers the truth. The key lesson is the importance of avoiding that first puff. How many marathon runners can run back-to-back marathons? Quitters need to be told the truth, that few quitters have the resolve to endure successive periods of withdrawal, even if educated and supported. It isn't a matter of weakness but brain function. One is too many, a thousand never enough!
Why is connecting with the entrenched smoker one of the greatest challenges known, yet once free many ex-smokers seem almost obnoxious in trying to get others to quit too? It evidences how horribly wrong they discovered they were, that nicotine addiction is about living a lie.
We need to teach smokers how nicotine hijacked their mind's priorities teacher, their dopamine pathways. We need to share the beauty of one of the greatest awakenings imaginable, traveling from deeply rooted convictions that life without smoking nicotine would be horrible and unthinkable, to discovery that everything we did while smoking can be done as well as or better without it.
Recovery isn't about strength or personal weakness. It's about arresting a brain priorities disease. It's about tasting calm and quiet once the addiction chatter ends.
Medications to Help You Quit - It's time to stop teaching nicotine addicts that nicotine is medicine. Clearly it requires more words to refer to NRT as "replacement nicotine" or an FDA approved quitting product. But simple doesn't make wrong right.
Whether the TCRB looks at NRT as gradual stepped-down nicotine weaning, or an opportunity to minimize physical withdrawal while permitting extinguishment of psychological use conditioning, at some point, if the quitter is to successfully arrest their underlying dependency, replacement nicotine use must end. Nicotine in NRT is identical to nicotine in tobacco. It's here that the NRT quitter benefits from the cold turkey quitter's play book. They too need teaching that replacement nicotine is fully capable of sustaining ongoing dependency, and of initiating relapse.
Clearly the pharmaceutical industry makes more money by referring to nicotine as medicine. In fact, they likely know that doing so creates confusion that hides natural learning of the Law of Addiction. Ask yourself, is it in the industry's financial interests to sell NRT only once, or to keep a smoker coming back to buy more?
Medicines That Help With Withdrawal - As discussed, this page's double "your" chances assertion is false. Additionally, the page is an informed consent liability nightmare. For example, readers are told that there are only two groups that Chantix "is not right for," those with kidney problems, or pregnant or breastfeeding women. That statement effectively tells smokers with a history of depression that Chantix is right for them.
Stress and Smoking - Again, the page's assertion and theme that "stress is a reason why many people smoke" has a tremendous following but absolutely no foundation in science (see "Why quitting is so hard," above). The reason they smoke is because they have a dependency rooted addiction. As taught in early Surgeon Generals reports, stress accelerates nicotine elimination, with replenishment restoring reserves.
Reasons for Quitting: Smoking's Impact on Others - This page opens by asserting that, "Even a little secondhand smoke is dangerous." Many smokers have smoking spouses, family members, friends or are exposed to smoke at work. Try to think like the smoker who has no choice but to endure some exposure. This gross overstatement of the degree of risk associated with "even a little" exposure can easily become fuel for junkie thinking that says, "If even a little is dangerous then what's the use in quitting?" While it may excite anti-smoking activists, telling a challenged quitter that "a little" secondhand is dangerous can facilitate relapse or cessation postponement.
Overview of Basic Steps - As discussed in detail above, asking quitters to "set a quit date" is contrary to the evidence base and likely doubles risk of relapse (see 2006 UK study and 2009 US study ).
Set a Quit Date - This page either invites cessation postponement or fuels gradually escalating quit date anxieties. Following this page's advice is likely to double risk of relapse (see 2006 UK study and 2009 US study ).
Talk to Your Doctor About Getting Help to Quit - A doctor's simple encouragement that their patient stop smoking generates a modest increase in odds of success regardless of quitting method. But this page isn't about putting your doctor on your support team. It's about belittling and discriminating against cold turkey cessation.
The page's primary objective is to have the doctor prescribe quitting "medicine" and could have been written by the pharmaceutical industry.
It opens with a hard slap of cold turkey quitting in suggesting that physicians do not support it. "Quitting 'cold turkey' isn't your only choice. Talk to your doctor about other ways to quit." Other ways? If the vast majority of Smokefree.gov visitors are quitting cold, isn't this page suggesting that it's a waste of time talking with their physician, as they support "other ways"?
Other Support - While quality support can more than double success rates, this page refers smokers to the 1-800-QUIT-NOW national telephone quitting line, which historically has been heavily scripted toward discouraging cold turkey quitting and supporting medication. What's seen at Smokefree.gov is fairly representative of the support advice currently being rendered at all levels of government. National cessation policy is in need of more than Internet window dressing. It screams for common sense and integrity analysis at all levels, especially telephone quitline counseling scripts.
Steps to Take on Your Quit Day - The primary theme of this page - telling smokers to avoid encountering as many cigarette use cues as possible - is not supported by science. It delays cue extinguishment. It also asks quitters to restructure their entire life, making recovery vastly more challenging than need be.
The only thing the smoker need do to succeed is to refrain from allowing nicotine back into their bloodstream. Instead of teaching smokers to fear and avoid their use cues and crave triggers, they need to know that meeting, greeting and extinguishing cues is a good thing, not bad. We should encourage them fully to embrace recovery, as each extinguished cue rewards them with return of another slice of life; the activity, time, location, person or emotion that generated the brief crave episode.
Recovery is about reclaiming life one extinguished use cue at a time. This page tells smokers to hideout in places where smoking isn't allowed, to listen to a different radio station, to take a different route home, to stop "watching your favorite TV show, sitting in your favorite chair or having a drink before dinner." Where is the cessation science backing cue avoidance as increasing success rates? It doesn't exist.
Additionally the page suggests that smokers benefit by adopting a host of new activities as substitutes for smoking including: exercise, holding something like a pencil, paper clip, or marble, or putting cinnamon sticks, lollipops, hard candy, sugarfree gum, or carrot sticks into their mouth. What evidence is there that adopting substitutes for smoking increases successful cessation?
To the contrary, smoking substitutes create risk that the new activity will become so intertwined with successful cessation that it becomes a psychological replacement crutch, a crutch that if suddenly removed can substantially elevate risk of relapse.
While exercise programs are normally beneficial, if adopted as a smoking avoidance technique and psychologically tied to successful quitting, what happens if the quitter sustains injury, illness or suddenly can no longer exercise? While healthy to exercise in order to control cessation weight gain, doing so as a smoking avoidance technique threatens recovery.
Find New Things to Do - As discussed immediately above, this page openly suggests to quitters that their odds of success are increased by adopting smoking replacement activities that "create some new habits." New habits? New habit replacement crutches will threaten relapse if leaned upon heavily and then suddenly removed. Quitters need not pick-up or give-up anything but nicotine to succeed.
Withdrawal: How You May Feel When You Quit - This page is about symptoms. Why is it necessary to mention and link to the medicines page when discussing withdrawal symptoms? Why no corresponding link that teaches cold turkey quitters how to minimize, without medicine, many of the listed withdrawal symptoms, including "trouble thinking clearly"?
The page lists 6 categories of withdrawal symptoms. It then states, "The medicines described in this guide can help." Help? Although vague, isn't the TCRB suggesting to quitters that medication can alleviate all six? Is it true?
What To Do If You Do Slip - As discussed, this page falsely suggests that most smokers who lapse are able to avoid full relapse. It's untrue! Asserting that smoking once is just a "small setback," that "one slip up does not make you a failure" is contrary to all relapse studies to date, contrary to the Law of Addiction, and provides junkie thinking fuel that falsely leaves readers believing that they can get away with smoking nicotine just once. The TCRB needs to ask itself, is this page costing lives?
Resources to Help You if You Slip Up - Although the page is simply a list of eight links, in its entirety it falsely suggests that most smokers are able to recover from a lapse, which is clearly untrue.
Closing Thoughts
Sadly, WhyQuit.com, with a marketing budget of zero, is Google's #2 ranked quit smoking site. Frankly, it shouldn't be. But with government health officials turning their backs, cold turkey quitters have nowhere else to go. It's our dream to witness the destruction of WhyQuit's popularity as the NCI and CDC at last fulfill their public health mandates, and service the cessation needs of America's cold turkey quitters.
A long shot, I hold out hope that this article clicks with some health policymaker who has the courage to speak their mind. I'm hoping that someone within the National Cancer Institute or its Tobacco Control Research Branch is willing to ponder the possibility that the current state of Smokefree.gov contributes toward costing cold turkey quitters their freedom, health and lives.
Real-world evidence shouts cold turkey's superiority over NRT, while NRT clobbers placebos inside clinical trials. Within the confusion, an army of paid industry consultants invents excuse after excuse in hopes of keeping health officials convinced to continue giving cold turkey quitters the silent treatment. But why? If truly motivated by concerns for smoker health, then what possible objection could there be to providing abrupt cessation quitters encouragement, education, counseling and support?
I dream that cessation health policymakers will start thinking for themselves, and rethink current policy. I hope they'll ask themselves, would providing quality support to America's millions of annual cold turkey quitters herald return of substantial annual reductions in the US smoking rate? How will we know unless we try? What do we have to lose?

{kind=link}
{kind=link}
{kind=link}