
National Cancer Institute quit smoking advice promotes cancer

How much and what quality of evidence is needed to establish whether National Cancer Institute (NCI) quit smoking advice is itself ineffective, thus diminishing successful quitting and ultimately costing lives?
The newest real-world smoking cessation study testing the hypothesis that nicotine replacement therapy (NRT) is ineffective, publication of Professor Simon Chapman's common sense book “Quit smoking weapons of mass distraction,” the NCI amending the National Health Interview Survey (NHIS) to ask about nicotine replacement while ignoring nicotine cessation, and numerous findings that nicotine promotes cancer, a rash of 2022 happenings beg a fresh and informed answer to the 38-year-old FDA advisory committee nicotine-dam-busting question, is Nicorette nicotine gum “a horror for the public health”?
“Double Your Chances”
To this day, the National Cancer Institute’s SmokeFree.gov website hammers visiting smokers and quitters with the message that “nicotine replacement therapy” is medicine that “can double your chances of quitting for good.”
A Google “Advanced Search” of SmokeFree.gov shows that the NCI’s “double your chances” medicine promise appears on 32 pages.
Does the word “your” suggest a quitter’s real-world chances or the odds of a smoker attracted to a six-month randomized placebo-controlled clinical trial (RCT) promising a 50/50 chance of getting weeks or months of free NRT or medication, a smoker willing to delay quitting until commanded to quit?
Limited to efficacy findings from RCTs, which have been plagued by an inability to blind quitters as to their assignment, contrary to NCI claims, neither the 2000 or 2008 U.S. Tobacco Treatment Guideline found that 6 to 14 weeks of nicotine gum “doubles” smoking cessation.
Instead, both found just 50% greater efficacy than placebo (2000 meta-analysis of 18 study arms, odds ratio, 1.5; 95% CI, 1.3-1.8 and 2008 meta-analysis of 15 study arms, odds ratio, 1.5; 95% CI, 1.2-1.7).
Newest NRT Findings
“Efficacy can be defined as the performance of an intervention under ideal and controlled circumstances, whereas effectiveness refers to its performance under ‘real-world' conditions” (Singal 2014).
The authors of Jackson 2022 open by noting that clinical efficacy doesn’t prove population-level effectiveness. A prospective real-world study to be published in the December 2022 edition of Addictive Behaviors, the study sought to prove the hypothesis that NRT is 25% less effective than quitting unaided. What it found was worse.
This was the same primary authors’ third look at NRT’s worth among UK quitters. Published in Mayo Clinic Proceedings, Kotz 2014 was a cross-sectional prospective analysis of population-level six-month quitting. It found that "Compared with smokers using none of the cessation aids" "use of NRT bought over the counter was associated with a lower odds of abstinence (odds ratio, 0.68; 95% CI, 0.49-0.94)."
In Jackson 2019 they compared 5,206 OTC NRT quitters to 8,348 unassisted quitters. They found that unadjusted smoking abstinence was 11.6% for OTC NRT users as compared to 16.8% for unassisted quitters.
Using a more prospective 12-month follow-up, Jackson 2022 found the unadjusted odds of quitting with OTC NRT were 43% lower than quitting unaided (odds ratio, 0.57, 95% CI, 0.39–0.84), and 40% lower for prescription NRT (odds ratio, 0.60; 95% CI, 0.37–0.98).
Although observational studies often adjust for potential confounders, as did these, SmokeFree.gov’s 32 “double your chances” promises and NRT commercials are unconditional. Unadjusted findings reflect "the full impact of real-world variability."
NCI Ignoring NRT Ineffectiveness
Do NCI “double your chances” NRT warranties simply reflect bureaucratic oversight? Twenty years of population-level ineffectiveness findings suggest otherwise.
First, the NCI has an entire division, the Tobacco Control Research Branch (TCRB), where part of the stated mission of its 16 employees is the dissemination of evidence-based findings to treat tobacco use in order to diminish tobacco-induced cancer and suffering.
The cancer-killing question is, who gets to define what "evidence-based" means, pharma and friends, or science?
Let’s dig deeper into the population-level NRT ineffectiveness evidence-base which the NCI and TCRB refuse to acknowledge or disseminate.
A 2002 Journal of the American Medical Association study surely set off alarms within the NCI. It concluded that "Since becoming available over the counter, NRT appears no longer effective in increasing long-term successful cessation in California smokers" (Pierce 2002).
Also in 2002, an observational study published in Addiction followed 2,367 OTC nicotine patch users, 2,981 OTC nicotine gum users, 269 prescription patch users, and 155 prescription gum users. It found an average 6-month smoking relapse rate of 93 percent (Shiffman 2002).
A London 2003 study found that among 1,845 smokers who had attempted quitting during the past 12 months, “willpower alone” quitters doubled the quitting rate of those who purchased NRT.
Alberg 2005 reported findings from 1,954 Maryland respondents who were current smokers in 1989 and provided follow-up data 9 years later in 1998. It found that “30% of NRT users compared to 39% of non-users had quit smoking, a statistically significant difference that persisted after adjustment for the sociodemographic characteristics and amount smoked.”
Doran 2006 examined successful cessation during the most recent quitting attempt of 3,135 Australian family practice patients surveyed in 2002 and 2003. Among 2,207 former smokers, 88% had quit cold turkey while only 9.5% had used NRT. The study also found that cold turkey doubled the nicotine patch success rate and was nearly 4 times as effective as nicotine gum.
Acknowledging that NRT use generally requires planning, West 2006 evaluated planned versus unplanned quitting among 918 smokers whose last attempt failed and 996 ex-smokers. It found 2.6 times higher odds of success for unplanned attempts than for planned ones (95% CI = 1.9, 3.6).
Featured in a 2007 front-page Wall Street Journal article entitled “Nicotine Fix,” Pulitzer Prize-winning journalist Kevin Helliker wrote, “An unpublished National Cancer Institute survey of 8,200 people who tried quitting found that at three months, users of the nicotine patch and users of bupropion remained abstinent at higher rates than did users of no medication. But at nine months, the no-medication group held an advantage over every category of stop-smoking medicine.”
Pouring cold water on its own “double your chances” promises, the unpublished and hard-to-find NCI study (Hartman 2006) has not been shared on any government website or referenced in any known NCI document.
Four of the authors of Ferguson 2009 were consultants to GlaxoSmithKline, the maker of Nicorette and Nicoderm. After surveying 900 U.S. smokers and 800 ex-smokers, they found that quitting product use was nearly 4 times more likely among those making planned attempts and that roughly 90% of unplanned attempts were made by cold turkey quitters. They also found that success during spontaneous unplanned attempts was more than double the rate for planned attempts (adjusted OR 2.62, 95% CI = 1.99, 3.45).
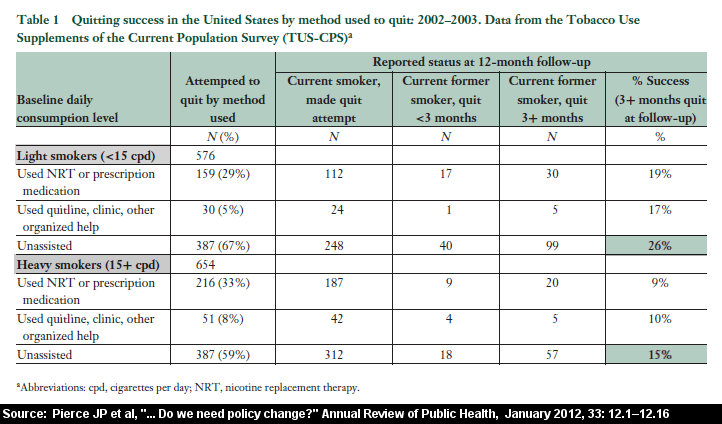
Pierce 2012 analyzed TUS-CPS survey data associated with 576 light smokers (<15 cigarettes per day) and 654 heavy smokers (>15 cigarettes per day). It found that in both groups, the quit smoking rate for unassisted quitters was significantly higher than for users of NRT or prescription medication.
Alpert 2012 was a 3 wave prospective cohort study of 787 Massachusetts smokers who had recently quit. It found that the odds of smoking relapse within the first six months were 3.5 times higher in heavily dependent quitters using NRT than in heavily dependent quitters not using NRT (95% CI = 1.50, 8.32).
A 2013 Gallup Poll found that most U.S. ex-smokers succeeded by quitting cold turkey, with just 1 in 100 crediting nicotine gum and only 8% crediting any approved stop-smoking product.
Leas 2017 was a propensity-matched effectiveness study using NCI 2002-2003 and 2010-2011 TUS-CPS survey data. Published in the Journal of the National Cancer Institute, after matching 12 potential confounders of 2,219 pharmaceutical aid users and nonusers, it found “no evidence that use of varenicline, bupropion or nicotine replacement increased the probability of 30 days or more smoking abstinence at one-year follow-up."
Table 7 data from Weaver 2018, a prospective population-based study evaluating 1,284 U.S. smokers recruited in 2015 and re-contacted one-year later, indicates that cold turkey was 3.3 times more effective and 11 times more productive than NRT.
Pierce 2020 was a 3 wave prospective PATH study following 2,443 U.S. daily smokers. According to Table 1 data, smokers quitting without any pharmaceutical aid (1,435) were 24% more likely to be abstinent from all forms of tobacco after 12 months, including e-cigarettes, than quitters using FDA-approved products (442). Also, unassisted quitting was 4.4 times as productive in generating ex-smokers as approved products (146 versus 33).
Heffner 2021 was a Veteran’s Administration medical records observational study of 47,609 screened smoking veterans receiving lung CT scans, where 8,337 received quitting medication within 30 days of the scan. According to Table 3, there was no difference in one-year quitting rates between veterans not using any quitting “medication” and veterans receiving single NRT (most “medication” quitters or 53%) or combination NRT (14.4%).
Don’t Quit Cold Turkey
The chapter 5 title in Professor Chapman's new bombshell book, the NCI’s TCRB hasn’t simply ignored and suppressed evidence of NRT's ineffectiveness, making a mockery of the Board’s mission statement. It's declared war on cold turkey, the path by which more nicotine-dependent humans successfully arrest their dependency and cancer risks than all others combined.
The TCRB mission statement doesn’t mention cigarettes. It identifies tobacco as the enemy. The tobacco industry has viewed nicotine as the sine qua non of tobacco use for at least 50 years.
The definition of “cold turkey” -- “abrupt complete cessation of the use of an addictive drug” -- doesn’t mention a particular method by which a drug enters the bloodstream.
A 2009 NCI evaluation of survey questions to be used in the 2010-2011 TUS-CPS survey included the question, “Would you say you tried to quit ‘cold turkey’ or in some other way?”
According to the interviewers, “Respondents had no difficulty understanding what was being asked of them in each of the above questions. Probes on the meaning of ‘cold turkey’ yielded correct answers without hesitation by respondents.”
The 2013 Gallup Poll found that most U.S. ex-smokers succeeded by quitting cold turkey. Doran 2006 found that among 2,207 Australian former smokers that 88% had quit cold turkey.
“Cancer Facts & Figures 2003” was published by the American Cancer Society. Table 3 (page 25) indicates that 91.4% of former smokers “Quit ‘cold turkey’ or slowly decreased the amount smoked.”
“Clearing the Air” is a 38-page quitting booklet published by the National Cancer Institute in 2008 that continues to be featured on the NCI website. Under page 10’s “Cold turkey” heading, the NCI actually “lies” to smokers and quitters about how most ex-smokers succeed.
There, the NCI tells them, “For some smokers, going cold turkey seems like the easiest way to quit: Just stop smoking and tell yourself you’ll never light up again. This works for some smokers—usually those with the lowest level of nicotine dependence—but not many. Fewer than 5 percent of smokers can quit this way.”
Professor Simon Chapman is the former editor of the BMJ journal Tobacco Control. Published in June 2022, Chapman’s free open access book “Quit smoking weapons of mass distraction” is an indictment of cold turkey bashing and quitting method productivity evidence suppression.
Chapman shares a UK NHS poster (also published in 2008) showing a man resisting a taught line tugging on a fishing hook that's penetrating his cheek. The first 2 lines of the caption read, "There are some people who can go cold turkey and stop. But there aren't many of them."
"When I first saw it I was gobsmacked by the outrageously incorrect statement," Chapman writes. "‘But there aren't many of them’ (who quit cold turkey) is completely and utterly wrong. It's a weapons-grade lie, which as we have seen is easily contradicted by data going back several decades to at least the 1960s."
And what representation does the NCI’s “Clearing the Air” make about NRT? You guessed it. Page 17 tells smokers that “Studies show that these medications, compared with trying to quit without them, can double or triple your chances of quitting for good.”
As for the TCRB’s cancer-fighting mission, to this day, even when the cancer patient is under the oncologist’s care and battling for their life, cold turkey is the NCI’s mission leader.
Bassett 2021 identified 151 smokers diagnosed with bladder cancer. After diagnosis 115 made a quitting attempt and 65 or 56% were successful. Among the 65 successful quitters, 42 or two-thirds (66%) quit cold turkey.
Santi 2022 followed 186 mostly heavy long-term smoking patients diagnosed with head or neck cancer. At six months, 13 patients had died and 41 had quit smoking. Among quitters, 51.2% quit cold turkey, while 14% used NRT.
SmokeFree.gov
The NCI’s SmokeFree.gov website ranks among the top three search results for the following Google search queries: quit smoking, smoking cessation, stop smoking, women smoking, quit vaping, dip tobacco, nicotine replacement therapy, NRT, and how to stop smoking immediately.
Notice what’s missing? SmokeFree.gov has its own internal search engine. A search of “cold turkey” returns the message, “Your search yielded no results.”
Reflect on the fact that the planet’s most productive quitting method isn’t mentioned on what may be the top-ranked quitting site. Neither are any of the above real-world quitting method effectiveness findings.
Smoke-Free.gov’s “Explore Quit Methods” reviews 13 quitting methods including the “Nicoderm CQ” nicotine patch, “Nicorette” nicotine gum, the “Nicorette” nicotine lozenge, the “Nicotrol” inhaler, and “Nicotrol” nasal spray. As if a joint GlaxoSmithKline and Pfizer NRT commercial, what’s odd is that manufacturers of NRT brands not mentioned aren’t demanding inclusion.
As troubling as cold turkey’s absence, SmokeFree.gov quitting tips and advice are generally tailored to support gradual NRT nicotine weaning schemes, not abrupt nicotine cessation.
West 2006 and Ferguson 2009 had nearly identical findings that unplanned spontaneous quitting is 2.6 times as effective as planned attempts. SmokeFree.gov delays the smoker’s impulse to quit by teaching quitters that “One of the keys to a successful quit is preparation. A great way to prepare to quit smoking is to create a quit plan.”
“Many smokers choose a date within two weeks to quit smoking. This will give you enough time to prepare. Really think about your quit date. Avoid choosing a day where you know you will be busy, stressed, or tempted to smoke.”
Catering to weeks or months of NRT gradual nicotine weaning, SmokeFree.gov actually downplays the significance of what it terms a “slip.”
Tempted quitters are greeted by the headline “Slips Happen.” “Quitting smoking is a process. It may take time. During that time, you might get frustrated. There’s a chance you might slip at some point and smoke a cigarette. Slips happen to a lot of people who quit smoking.”
The suggestion that lots of successful quitters slip doesn’t just invite relapse, it’s contrary to lapse/relapse evidence.
Garvey 1992 followed 235 adult smokers for a year after attempting to quit. It found that "Those who smoked any cigarettes at all in the post-cessation period (i.e. lapsed) had a 95% probability of resuming their regular pattern of smoking subsequently."
Brandon 1990 found that "The high rate of return to regular smoking (88%) once a cigarette is tasted suggests that the distinction between an initial lapse and full relapse may be unnecessary."
Ongoing NRT use prevents SmokeFree.gov from sharing practical abrupt nicotine cessation advice such as a basic timeline of how long it takes for the body to become nicotine-free, how long before peak withdrawal passes, and how long before down-regulation and re-sensitization of brain dopamine pathway receptors.
It prevents teaching cold turkey quitters how to minimize common abrupt cessation symptoms, how blood-serum caffeine levels double after ending nicotine use, or the critical lesson that nicotine addiction is permanent and that just one puff after quitting and up to 50% of brain dopamine pathway receptors become occupied by nicotine.
Most importantly, the NCI misses a golden opportunity to advance natural lapse/relapse learning. It’s the eventual realization that there was always only one quitting rule, that while one puff will always be too many and thousands not enough, it’s impossible to fail so long as all nicotine remains on the outside.
2022 National Health Interview Survey
Enacted by Congress in 1956, the purpose of the National Health Survey Act was to learn about the state of health of Americans via annual and special surveys asking questions about the diseases and conditions afflicting them, including cancer, and for “adequate planning of any programs to improve their health.”
What better means to discover how most Americans succeed at the TCRB’s mission of “tobacco” cessation than to ask?
In 2021, 87,500 adults participated in National Health Interview Survey (NHIS). Beginning with the 2022 NHIS, the National Cancer Institute is co-sponsoring 16 new quit smoking method questions that will be asked biennially.
Guess which method the NCI doesn’t ask about? Yep, America’s most productive.
The (1) nicotine patch, (2) nicotine gum or lozenge, (3) the nicotine nasal spray or inhaler, (4) Chantix, (5) Zyban or Wellbutrin, (6) counseling, (7) a telephone quitline or (8) a stop smoking clinic or support group, eight questions will ask about the quitting methods used during the past 12 months, and eight will ask about the method used during the smoker’s final successful attempt.
No NCI cold turkey survey question in a decade, so what's the critical missing question?
“Thinking back to when you stopped smoking completely, did you … abruptly and completely end the use of all products containing nicotine (cold turkey)?
The “core” annual NHIS survey already asks two e-cigarette questions, including “Do you now use e-cigarettes or other electronic vaping products every day, some days, or not at all?”
Thus, a single abrupt nicotine cessation question would instantly exclude and expose all nicotine shell game participants including nicotine replacement, transfer or switching, gradual nicotine weaning or tapering, or use of new nicotine products such as IQOS, including delivery devices not yet invented.
Consistent with the TCRB’s “tobacco” cessation mission, it would bring a laser focus to the long-neglected research question, what is/are the keys to successful abrupt nicotine cessation?
The problem is that asking it would instantly expose “Clearing the Air” as anything but. The most traveled smoke-free path, asking it would make glaring SmokeFree.gov’s “cold turkey” omission. Asking it would compel the NCI to, at last, acknowledge NRT’s ineffectiveness or at least stop suppressing effectiveness findings.
Whether NRT, e-cigs, or IQOS, the root problem is that establishing cold turkey’s contribution to national smoking cessation or nicotine dependency recovery is contrary to a trillion-dollar nicotine industry’s economic interests.
The NCI could have asked a single NRT use question or a single approved quitting product question. Instead, it asks ten. Who stands to benefit? Unlike SmokeFree.gov listing only GlaxoSmithKline and Pfizer NRT brands, NHIS NRT questions don’t mention brands.
TUSCS – CPS
It isn’t like the NCI hasn’t previously asked cold turkey questions. The NCI’s 2002-2003 and 2011-2012 Tobacco Use Supplements to the Current Populations Survey (TUS-CPS) asked about cold turkey in three different situations: (1) during the smoker’s most recent attempt, (2) when they stopped smoking completely all at once and (3) during attempts to quit smokeless tobacco, pipes or cigars.
For example, the 2010 and 2011 TUS-CPS asked:
Did you try to give up cigarettes all at once?
(1) Yes (2) No
When you tried to quit all at once, would you say you tried to quit “cold turkey"?
(1) Yes (2) No
IF NEEDED: “COLD TURKEY” IS STOPPING ALL AT ONCE WITHOUT ANY AIDS.
The TUS-CPS also asked about NRT use in the same three situations. For example:
Thinking back to the last time/time you tried to quit smoking in the past 12 months. Did you use any of the following products:
(1) Yes (2) No
A nicotine patch |__|
A nicotine gum or nicotine lozenge |__|
A nicotine nasal spray or nicotine inhaler |__|
Thus, unlike the NCI’s 2022 NHIS 2022 survey questions which exclude the nation’s most productive nicotine dependency recovery method, a decade earlier, at least the NCI was asking.
A Google search and study search attempting to locate any discussion of 2002-2003 or 2011-2012 TUS-CPS cold turkey findings, or how cold turkey compared to NRT, failed.
While the NCI's unpublished Hartman 2006 analysis of 2003 TUS-CPS findings mentions NRT 68 times, cold turkey isn't mentioned. It's as if no NCI cold turkey question has ever been asked.
NCI Cancer Promotion
According to the NCI, “Tobacco use is a leading cause of cancer and of death from cancer.”
“Tobacco use causes many types of cancer, including cancer of the lung, larynx (voice box), mouth, esophagus, throat, bladder, kidney, liver, stomach, pancreas, colon and rectum, and cervix, as well as acute myeloid leukemia.”
The NCI advises that “People who use any type of tobacco product are strongly urged to quit. People who quit smoking, regardless of their age, have substantial gains in life expectancy compared with those who continue to smoke. Also, quitting smoking at the time of a cancer diagnosis reduces the risk of death.”
And where does the NCI refer smokers wishing to quit? SmokeFree.gov, Clearing the Air, and NCI telephone quitlines that promote NRT while strongly discouraging cold turkey.
Roughly half of adult smokers smoke themselves to death. Nearly all population-level evidence declaring NRT ineffective while the NCI shouts that it doubles “your” chances, the conclusion that current NCI smoking cessation advice promotes cancer seems inescapable.
But that’s not the only way that the National Cancer Institute’s cessation policy promotes cancer. So far, at least eleven 2022 studies have sounded nicotine cancer-promotion alarms.
- "Lung cancer is the leading cause of cancer-related death worldwide." "It has been found that nicotine can induce resistance to chemotherapy and radiation in a number of tumors by activating a range of intracellular signaling pathways and promoting angiogenesis." "The results of the present study demonstrated that nicotine upregulated miR-21-3p in lung cancer cells, leading to suppression of the proapoptotic protein FOXO3a and subsequent proliferation of tumor cells, therefore resulting in chemoresistance." (Oncology Letters 2022)
- “Triple negative breast cancer is more aggressive than other breast cancer subtypes ..." “We ... detected that nicotine significantly reduced the increase in cell apoptosis induced by paclitaxel treatment. Moreover, the presence of nicotine reduced the efficacy of paclitaxel treatment administered in three cycles to MDA-MB-231 tumor cells.” (World Journal of Clinical Oncology 2022)
- "Oral squamous cell carcinoma (OSSC) is a common malignancy affecting 30,000 people in the United States each year. Our objective was to determine the impact of eCig and nicotine on gingival OSSC invasion and their secretion of pro-inflammatory molecules." "These results support the already established data showing that nicotine promotes oral carcinogenesis." (Frontiers in Oncology 2022)
- "Collectively, our results depicted a novel and clinically important mechanism of chemoresistance in small cell lung cancer (SCLC) treatment: nicotine exposure significantly compromises the efficacy of platinum-based chemotherapies in SCLC treatment by reducing therapy-induced DNA damage and accelerating chemoresistance acquisition. The results also emphasized the urgent need for tobacco cessation and the control of NRT use for SCLC management." (Cancers 2022)
- "We propose that E-cig nicotine can be nitrosated in mouse and human cells becoming nitrosamines, thereby causing two carcinogenic effects, induction of DNA damage and inhibition of DNA repair, and that e-cigarette aerosol is carcinogenic in mice." (Mutation Research 2022)
- "Nicotine, a psychoactive alkaloid found in tobacco, is associated with the development of gastric cancer." (International Journal of Molecular Sciences 2022)
- “Nicotine … promotes angiogenesis, proliferation, and epithelial-mesenchymal transition while promoting growth and metastasis of tumors." "Nicotine contributes to the pathogenesis of a wide range of cancers including breast cancer through its carcinogens such as NNK and NNN." (Breast Cancer 2022)
- “From the present study, it could be concluded that nicotine significantly induced rectal cancer in the mice model by modulating gut microflora and increasing COX-2 and prostaglandin E2 levels.” (Turkish Journal of Gastroenterology 2022).
- "Brain metastasis is the most common malignancy of the central nervous system, occurring in up to 50% of lung cancer patients with a median survival of less than a year and at a rate twice to ten times higher than that of primary neural neoplasms." "Here, we showed that nicotine skews neutrophil polarization within the pre-metastatic brain niche and promotes metastatic colonization of lung cancer cells by regulating their stemness and energy metabolism." (Oncogene 2022)
- "Nicotine enhances proliferation, angiogenesis and metastasis and inhibits apoptosis/autophagy in [non-small cell lung cancer] cells by activating nicotinic acetylcholine receptors (nAChRs), especially the α7 subunit, and its downstream signaling pathways ..." (International Journal of Molecular Sciences 2022)
- "Nicotine, the most abundant smoke component, deposits on indoor surfaces during smoking and reacts with pollutants in the indoor environment to form a mix containing toxic and carcinogenic chemicals. More specifically, surface-bound nicotine reacts with nitrous acid (HONO), a common atmospheric species that is emitted from indoor combustion appliances and smoking, to produce tobacco-specific nitrosamines (TSNAs) including NNA, NNK and NNN." (PLoS One 2022)
The National Cancer Institute’s silence on the fact that nicotine promotes cancer is deafening.
Does NCI cancer screening or cancer treatment guidance warn smokers that any form of continuing nicotine use, including NRT or e-cigarettes, diminishes the ability of radiation or chemotherapy to kill cancer cells?
The NCI conducts the Health Information National Trends Survey (HINTS) which routinely sample’s “the American public's use of cancer-related information.” An October 2018 Hint’s Brief reported that “49 percent of Americans incorrectly believe that nicotine causes most smoking-related cancers.”
Clearly, a huge chunk of America correctly believes that without nicotine people wouldn’t smoke and smoking-related cancers wouldn’t occur.
Clearly, the NCI was fully aware in October 2018 of the multiple ways by which nicotine promotes cancer, yet chose to play HINTS cause/promote word games in squashing all nicotine-cancer beliefs instead of correcting them.
In June 2015, the NCI sponsored the “Smoking Cessation at Lung Examination” (SCALE) collaboration, funding 7 randomized low-dose computed tomography clinical trials involving long-term smokers (30+ years), smokers most likely to develop lung cancer. At least 8 study arms were described as receiving NRT.
What about participants whose CT scans result in cancer concerns? Surely, the Institutional Review Board approving the study would declare that replacement nicotine use by them was contraindicated.
Despite awareness that up to 60% of low-dose CT scans locate abnormalities, with up to 56% requiring tracking, the only “Informed Consent” form available online that’s associated with the NCI-funded studies doesn’t mention how NRT use will be handled when a CT scan reveals nodules.
What about e-cigarette use? There, the NCI tells smokers visiting SmokeFree.gov, “So far, the research shows there is limited evidence that e-cigarettes are effective for helping smokers quit.”
Yes, the NCI finds “some” evidence of effectiveness associated with switching to e-cig nicotine but zero mention of the undisputed king of nicotine cessation.
Does the nation’s cancer prevention guardian share the fact that vaping nicotine promotes cancer? No.
SmokeFree.gov’s e-cigarette risks review mentions only the possibility of addiction, fetal harm, adolescent brain development concerns, and the possibility of inhaling harmful chemicals other than nicotine.
Why?
Faced with a mountain of evidence that gradual nicotine weaning doesn’t work and that nicotine promotes cancer, why does the National Cancer Institute promote nicotine replacement and switching games but not nicotine cessation?
Occam's Razor suggests that “the simplest solution is almost always the best.”
This article presents substantial credible evidence suggesting that the NCI isn’t serious about battling the leading cause of cancer death worldwide. But why?
The NCI is people. Have you noticed how MSNBC and Fox News have super-polarized U.S. politics? When it comes to the influence and “group-think” objectives of a trillion-dollar nicotine industry, are NCI employees any less susceptible?
Why does Phillip Morris USA’s Quit Assist website teach smokers that NRT is a “key” to successful quitting, that “Nicotine Replacement Therapy (NRT) medications provide small, steady doses of nicotine to help stop cravings and relieve symptoms people might experience while trying to quit smoking. Some NRTs are available without a prescription, including gums, inhalers, nasal sprays, lozenges, and patches.”
Why in 2021 did Philip Morris International purchase a pharmaceutical company that makes nicotine gum, tablets, and powders? Why is a subsidiary of cigarette giant Reynolds American selling cinnamon Zonnic nicotine gum?
And have you ever wondered why no GlaxoSmithKline or Pfizer quitting product commercial has ever mentioned why it’s important to quit, that smoking kills?
I could devote as many words again to NRT industry NCI influence. Simply put, over the past three decades, an army of pharma-paid PhD consultants have successfully molded and manipulated NCI NRT beliefs.
Will the evidence shared above change things? No. But a four-time NRT failure myself, one last time, in memory of Neal Curtis (53) and Helen Bradford (50), and millions of unnamed NRT-trusting cancer victims, I had to try.
 John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," and 6 peer-reviewed journal articles. John is the founder and director of Turkeyville, a 15,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com
John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," and 6 peer-reviewed journal articles. John is the founder and director of Turkeyville, a 15,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com

{kind=link}