
Australia's half-baked quit smoking campaign
Does coerced smoking cessation work, or will the world's most expensive cigarettes further expose nicotine addiction's true depth and grip? And how do we square the planet's most repulsive cigarette prices and packs with its worst quitting method advice? Is the Australian government intentionally trying to keep smokers enslaved and paying?

Australian Cigarette Pack Prices
Zero cigarette advertising nationwide, logo-less and colorless cigarette packs totally void of branding, nearly the entire pack devoted to a disturbing smoking health risk image, and already the second highest cigarette pack-price of any nation, at first blush Australia appears deadly serious about smoking cessation.
But is it? For smokers, things are about to get worse.
Starting tomorrow, the federal tax on a pack of Australian cigarettes will jump 12.5 percent. Additional tax increases coming, it won't be long before Australian cigarettes likely become the the world's most expensive. It's expected that this initial increase will cost the average smoker about $10 more per week, roughly $2.00 more per pack.
The exact amount will depend upon how much cigarette makers increase prices above the tax increase, in order to protect income and shareholders from an expected decline in sales.
The last cigarette tax incease was 25% in 2010. It raised the price of a pack of 30 cigarettes by $2.16 and triggered a 70% spike in quitting attempts. Australian smokers face an additional 12.5% tax increase each year for the next three years. Together, they are expected to increase the yearly cost for the average smoker from $5,000 in 2013 to $7,000 by 2016.
History has taught governments to expect a price increase of 10% to lead to a decrease in cigarette sales of 3 to 5 percent. According to CNN, a 62-cent-per-pack 2009 U.S. federal tax increase resulted in a 10 percent decline in cigarette sales. But much of the decline is smokers smoking fewer cigarettes more intensely.
Earlier this year, President Obama called for a 94-cent-per-pack cigarette tax increase to fund universal pre-kindergarten, a move that would nearly double the federal cigarette tax from $1.01 per pack to $1.95. According to a July 2013 price survey, pack prices in the continental U.S. average $6.50, with a low of $4.96 in Kentucky to a high of $14.50 per pack in New York. How does $6.50 compare to world prices?
According to an August 1, 2013 UK Guardian story, as measured in U.S. dollars, Norway then had the world's highest price per pack at $15.11, followed by Australia at $12.14, the United Kingdom at $10.99, Ireland $10.92, Canada $10.51, New Zealand $10.35, Singapore $9.29, France $8.31, Switzerland $8.28, Iceland $8.23, Sweden $7.74, Finland $7.61, Netherlands $7.21, Belgium $6.97, Denmark $6.94, Germany $6.86, Italy $6.48 and Belize at $6.39.
A July 2013 study found that 87.5% of Australian smokers said they would seriously consider quitting if each cigarette reached a cost of one dollar. But would they? Does coerced cessation work as well as advocates suggest?
While a November 2013 Philip Morris study fixed Australia's adult smoking rate at 20.4%, the Australian Bureau of Statistics puts the rate at 16.3%. By contrast, here in the U.S., where cigarettes cost half as much, where there is no smoking harm picture on any fully-branded pack, and where stores are busting at the seams with smoking advertisements, the CDC places the U.S. smoking rate at 18%.
Nicotine Addiction Real Drug Addiction
On the eve of Australia's tax increase, the Sydney Morning Herald quotes quit smoking clinic director Dr. Colin Mendelsohn as saying, "I really think that it's exploiting smokers - who are drug addicts - who want to quit but can't." Can't?
There is increasing recognition that nicotine dependence reflects real drug addiction, a brain wanting disorder. The nicotine addict's wanting and urges flow from the same brain dopamine pathways as the wanting felt by the alcoholic and by opiate, cocaine and methamphetamine addict. The mind's nicotine compromised survival instincts teacher has assigned smoking nicotine the same use priority as it assigns to eating food.
According to Dr. Nora Volkow, director of the U.S. National Institute on Drug Abuse, "drug addiction is a mental illness. It is a complex brain disease characterized by compulsive, at times uncontrollable drug craving, seeking, and use despite devastating consequences - behaviors that stem from drug-induced changes in the brain."
Scientists have documented how nicotine physically alters the brain. Nicotine activates, saturates and desensitizes dopamine pathway receptors, which is followed by growth or activation of millions of extra receptors, a process known as up-regulation.
One cigarette per day, then two, then three, the longer nicotine is smoked, the more receptors become saturated and desensitized, the more grown, and the more nicotine needed to satisfy resulting "want" for replenishment.
Does there come a point with cigarette price increases where health ethics demand that the cost-benefit analysis factor in the full price paid by families of those least able to afford a parent inhaling the world's most expensive nicotine, including babies and children going without milk or child support?
Does the intentional creation of unbearable prices among the 2.8 million Australian's living in poverty impose a moral obligation upon government to educate them about cheaper and less destructive forms of nicotine delivery?
Cold Turkey Australia's Quitting Method Champ
Australian health officials continue to force feed their nation's highly motivated quitters replacement nicotine despite every long-term independent population level quitting method study over the past decade finding that it undercuts successful quitting.
Replacement nicotine is rooted in the belief that smokers can wean themselves off of nicotine. While successful gradual stepped-down nicotine reduction is more likely to succeed in contact rich clinical studies, few real-world quitters have a dozen or more quitting session appointments calendared with gradual weaning experts.
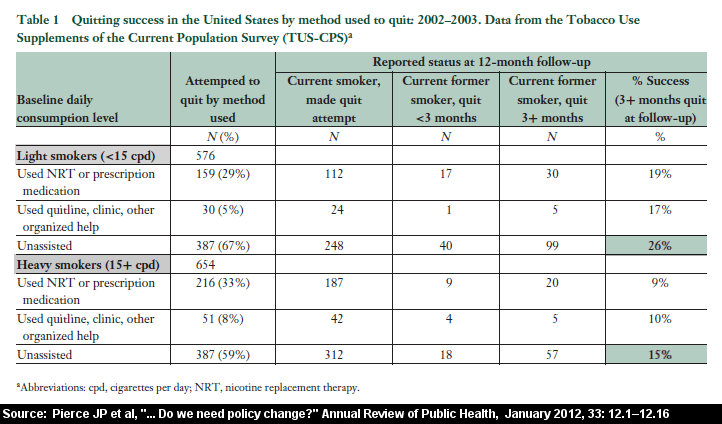
A 2007 survey, which included Australian quitters, "found that smokers who used the cold-turkey method to quit were almost twice as likely to abstain for a month or more in their attempt" as those using a gradual reduction or cut-down method.
A 2006 Australian study analyzed the smoking patients of 1,000 family practice physicians. It found that a whopping 88 percent of successful ex-smokers quit smoking cold turkey. It also found that success rates among cold turkey quitters were roughly double the rates of those using the nicotine patch, gum, inhaler or Zyban.
A 2012 review found NRT ineffective regardless of whether the person was a light or heavy smoker.
A 2013 U.S. Gallup Poll found that after three decades of nicotine gum marketing and billions spent on advertising, that only 1 in 100 ex-smokers credited nicotine gum for their success. And when all approved quitting products are combined, only 8 in 100 credit any form of approved quitting product, including Champix (Chantix in the U.S).
Clearly, the tail is not only wagging the dog, it's killing it.
As expected, the Poll also found that cold turkey accounted for more successful quitters than all other quitting methods combined.
If true, what possible motivation could Australian health officials have for steering Australian quitters toward the least effective quitting method, while bashing and trashing cessation confidence in the best?

As indicated above, cold turkey has continued to prevail since this 2013 article was written. Click the image to learn about this study and others.
Official Australian Quit Smoking Policy
As in many nations, pharmaceutical financial influence owns official government quit smoking policy. The Australian Government Department of Health is no exception.
The Australian government refers doctors seeking guidance on how to help smoking patients quit to an 80 page 2011 document entitled "Supporting smoking cessation: a guide for health professionals."
PDF page 2 of the "Guide" openly admits that it was bought and paid for by GlaxoSmithKline, maker of Nicorette and Nicoderm quitting products. Additionally 3 authors of the "Guide" admit to having previously accepted money from Pfizer (which sells Champix) or GlaxoSmithKline.
PDF page 19 of the Guide tells doctors and other health care providers that:
"Pharmacotherapy is recommended for all dependent smokers who express an interest in quitting, except where contraindicated."
Doctors are told that "first line options are medicines that have been shown to be effective" and in "Australia these are NRT (brands include Chemist's Own Nicotine, Nicabate CQ®, Nicorette®, Nicotinell®, QuitX® and others), varenicline (brand name Champix®) and sustained release preparations of bupropion hydrochloride (brand names Buproprion-RL™, Clorprax®, Prexaton and Zyban SR®)."
PDF page 29 tells physicians that "all forms of NRT (at equivalent doses) are similarly effective in aiding long term cessation," that "all forms of NRT can increase the rate of quitting by 50-70 percent."
Not once does the Guide warn doctors that NRT's 50-70% rate reflects efficacy over placebo, findings from studies that we now know were not blind as claimed.
How many times does the Guide mention the 2006 Australian study which found that nearly all successful patient smoking cessation was via cold turkey (88%)? None.
Instead, PDF page 41 of the Guide discourages cold turkey:
"Although many smokers are likely to attempt quitting unassisted, this approach has a low likelihood of succeeding (3-6% success rate) on any given attempt."
Three to six percent sounds totally unacceptable. And that's clearly the comment's intent.
Does the Guide share with doctors the comparable over-the-counter replacement nicotine one-year real-world continuous cessation rate, ineffectiveness reflected in the July 2013 Gallup Poll finding that only 1 in 100 successful quitters used nicotine gum? No. Doing so would totally undermine the Guide's objectives.
While PDF page 63 of the Guide includes Internet links to GlaxoSmithKline, Pfizer and Johnson & Johnson quit smoking support sites, despite the fact that more Australian smoking patients attempt cold turkey than all other methods combined, the Guide does not contain any link to any free cold turkey resource such as WhyQuit, Turkeyville or Joel's Library.
QuitNow.gov.au Really BuyMeds.now
Like the Guide, the Australian government's QuitNow.Gov.au website is drenched in pharma influence and dripping nicotine. Interestingly, the site actually grows the Guide's 50-70% NRT success rate.
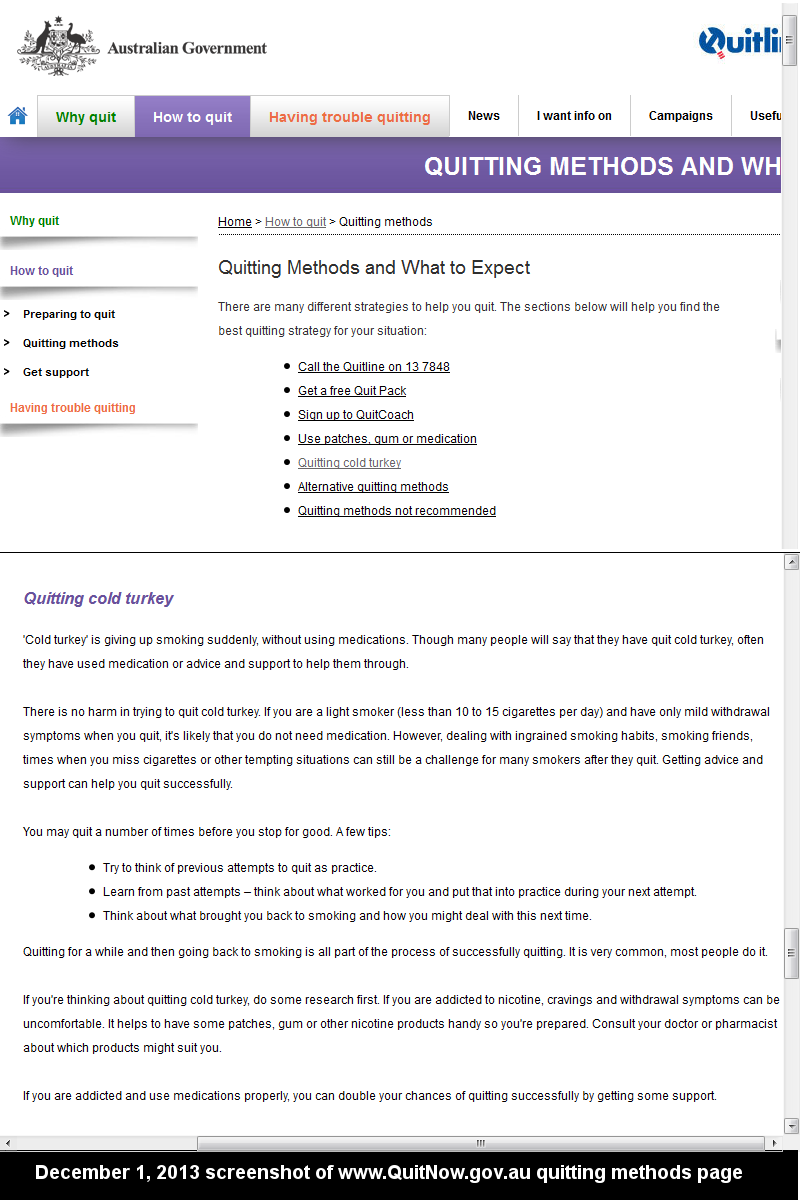
Smokers and quitters visiting QuitNow's Quitting Methods page (12/01/13 screenshot) are told that:
"Research shows if you're addicted to smoking and use these medications properly, you can double your chances of quitting successfully."
The word "your" clearly implies population level effectiveness over how most smokers normally attempt to quit (cold turkey), not clinical efficacy over a quitter who joined a study seeking free medication, but who was given a look-a-like placebo quitting product instead.
The good news is that unlike the Guide, QuitNow's Quitting Methods page actually has a heading entitled "Quitting Cold Turkey." The bad news is that after reading it, Australian cold turkey quitters can't help but walk away totally discouraged.
The section opens by suggesting that successful cold turkey quitters either cannot remember how they quit or are liars.
"Though many people will say that they have quit cold turkey, often they have used medication ..."
Imagine government's primary advice to cold turkey quitters including the message that failure is normal and expected.
"Quitting for a while and then going back to smoking is all part of the process of successfully quitting. It is very common, most people do it."
Unbelievably, Australian health officials next tell cold turkey quitters to buy and keep replacement nicotine handy, even if quitting cold, just in case things get uncomfortable.
"If you're thinking about quitting cold turkey, do some research first. If you are addicted to nicotine, cravings and withdrawal symptoms can be uncomfortable. It helps to have some patches, gum or other nicotine products handy so you're prepared. Consult your doctor or pharmacist about which products might suit you."
Is this nicotine tease cold turkey sabotage attempt intentional? Not discussed is that within 72 hours of ending all nicotine use that cold turkey quitters become 100% nicotine-free and move beyond peak withdrawal. Frankly, it's unconscionable that any government quitting site would suggest that cold turkey quitters put themselves through nicotine detox twice.
And how does the Australian government conclude its advice on successful cold turkey quitting? By falsely suggesting to every cold turkey quitter reading the section that unless they use medicine that they are twice as likely to fail.
"If you are addicted and use medications properly, you can double your chances of quitting successfully by getting some support."
How can a nation hell bent on motivating cessation via the planet's highest cigarette taxes demonstrate such gross incompetence in discouraging and demoralizing the quitter's natural instinct to end nicotine use, instead of finding creative ways to replace it?
Having become dependent upon cigarette taxes and in need of an additional $5.3 billion, are we witnessing the world's largest government health conflict of interest?
If replacement nicotine is in fact vastly less effective than quitting without it, is it fair to suggest that the current Australian government tobacco control policy is designed to keep smokers hooked and paying through their teeth? You be the judge.
I, John R. Polito, am solely responsible for the content of this article. Any error brought to my attention will be immediately corrected.

{kind=link}
{kind=link}