
JAMA Study Concludes NRT Ineffective
A new nicotine replacement therapy (NRT) study entitled "Impact of Over-the-Counter Sales on Effectiveness of Pharmaceutical Aids for Smoking Cessation" was published today in the Journal of the American Medical Association (JAMA). Its authors, John P. Pierce, PhD and Elizabeth A. Gilpin, MS, conclude that: "NRT appears no longer effective in increasing long-term successful cessation in California smokers."
Although I deeply admire the courage of any researcher who dares publish scientific findings contrary to the financial interests of the rich, powerful and influential neo-nicotine industry (pharmaceutical companies), I respectfully submit that their conclusion is wrong. I submit that NRT was "never" truly "effective" in helping California smokers quit, or any quitters for that matter.
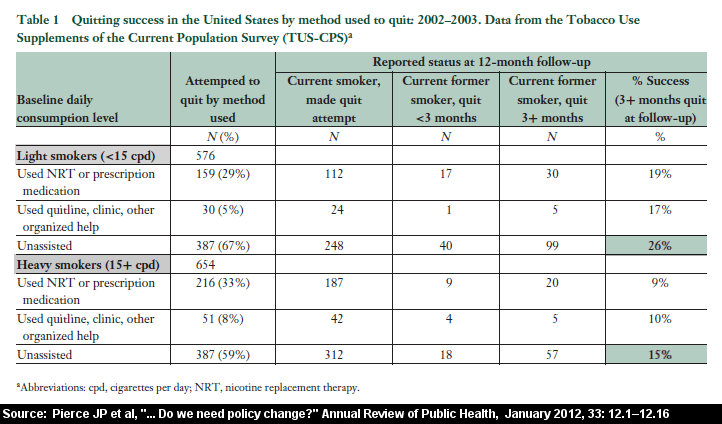
Pierce and Gilpin analyzed data from some of the largest tobacco surveys ever conducted, the California Tobacco Surveys (CTS) of 1992, 1996, and 1999. They knew that in 1996 the FDA approved the over-the-counter sale of both nicotine gum and patches and that both quickly became widely available. The CTS data indicated that NRT use skyrocketed by 50.5% from 1992 to 1999. The 1999 data indicated that 17.2% of California quitters had used either the nicotine patch (10.7%), nicotine gum (5.4%), an antidepressants such as Zyban/Wellbutrin (5.2%), or a combination, during their most recent attempt at quitting.
This is a link to a free full text copy of the Pierce JAMA study. Enlargement and close examination of the three 1999 graphs leaves one wondering how pharmaceutical companies can keep a straight face while taking a quitter's hard earned money before robbing them of their hope, spirit, confidence, precious cessation opportunity, and very possibly their life. According to the study's graph for "moderate to heavy smokers" (defined as those smoking 15 cigarettes or more per day), within 180 days or six months of quitting the percentage who had relapsed while quitting with the patch or gum was ever so slightly higher than those quitting on their own. Higher! Among light smokers (less than 15 per day) those using NRT and/or antidepressants like Zyban or Wellbutrin were relapsing at a slightly higher rate than the cold turkey quitters within just 90 days or three months of quitting. Again, slightly higher! But why?
Zero Benefit for Light Smokers
Before looking at the question of "why" 1999 California NRT quitters performed ever so slightly worse than those quitting on their own, I'd like to quote one of the most important findings from the study that relates to "light smokers" - those smoking fewer than 15 cigarettes per day.
"In 1999, no advantage for pharmaceutical aid users was observed in either the short or long term for the nearly 60% of California smokers classified as light smokers."
Imagine a two month clean-nicotine gradual withdrawal program where within just three months you're doing a bit worse than if you'd simply quit on your own. Studies had already shown that NRT was a total waste for teenagers smoking an "average" of 20 cigarettes a day or less , but the California data indicates it's a waste for all smokers. At least the heavy smoker who transferred to clean-nicotine enjoyed a couple of months of doing better (not smoking), than they otherwise would have, before their own natural quitting abilities surpassed science's latest quick fix magic cure - more nicotine.
U.S. Government Knew
Like an ostrich with its head in the sand, the U.S. government knows that tobacco is killing off Americans at the rate of almost a half-million per year ( 480,000 ), that NRT has been widely available for nearly three decades, and that the vast majority of quitters have tried quitting with NRT and failed. It also knows full well that its very own national cessation figures are very much in line with those published in Pierce's California JAMA study; that NRT is a sham, that 46 million adults smoked nicotine in 1994 and that 42 million smoke twenty years later.
The U.S. Department of Health, the U.S. Surgeon General, the CDC, the FDA, and the National Institute of Health all already knew that NRT was a national flop on the very day that the government published the June 2000 U.S. Guideline . But the neo-nicotine pushers had already taken over national cessation policy and there was no stopping their profit driven nicotine selling campaign. These guys are far more intelligent and creative than the tobacco companies ever were.
They are on the inside, writing U.S. policy, and the entire show now belongs to them. Every advantage is theirs to command and I'm sure they'll continue to enjoy pulling the strings of all U.S. health bureaucrats, together with the strings of national health and tobacco control organizations, which have been bought and paid for with cash.
Over-the-Counter Study Findings Ignored
Over-the-counter (OTC) NRT products are today generating mid-year cessation rates in the 8 to 11% range (see Davidson OTC 1998 , Hays OTC 1999 , Hurt Youth NRT 2000 , Shiffman OTC 2002 ). In other words, 89 to 92% of OTC NRT users are relapsing within six months. When the early non-OTC studies were released, NRT appeared to be performing a bit better. What actually happened and why were the 1992 California rates more in line with the early NRT studies? Did the early studies truly measure NRT's effectiveness? Is the title of the Pierce and Gilpin 9/11/02 JAMA study article well named in that over-the-counter NRT sales did have an impact upon NRT effectiveness rates, or did the early studies and California's early returns (1991) simply not reflect NRT's true ineffectiveness? Did they instead allow NRT to temporarily hide behind the enthusiasm of excited physicians and pharmacist who gradually learned that NRT was not the highly effective magic cure originally promised? Did the early studies allow NRT to hide behind layers of study protocols , including high quality behavioral components, into which those using NRT were thrust?
"Nonsense," say the experts, "those in the placebo group received the exact same behavioral training and were subjected to identical protocols!" Rubbish. In most NRT clinical studies the vast majority of the nicotine starved placebo group relapsed within a week (examples: 60% with a week, 80% within two weeks and 81.7% within three). The well-fed NRT group continued receiving the long-term benefit of further instruction, counseling, support, follow-up reinforcement, study perks and were bathed in ongoing university study protocols that left them feeling genuinely supported.
Treated the same? I don't think so. In most cases the studies were bought and paid for with pharmaceutical company dollars and the behavioral training and study protocols were often geared toward achieving success for those attempting to slowly wean themselves of all nicotine by gradual nicotine withdrawal. Does anyone believe for a moment that the chemically deprived nicotine addict (placebo users) and the well fed addict (NRT users) shared the same cessation experience or had the same needs at the same time? Who would you design your study to support?
No Requirement to Complete Therapy
Another study flaw was that if the NRT quitter got tired of the gradual withdrawal game, came to their senses, tore off their patch on day two, and went it alone and succeeded in quitting, that the study awarded full credit to "therapy" and zero credit to the quitter. If nicotine replacement therapy is truly "therapy," and not just a new tobacco company competitor, why does no study require NRT quitters to complete a minimum amount of therapy (at least 3 days) before claiming full credit for their victory? The protocol flaws of most early NRT studies are deep. In fact, they go to the very core of all "cessation" study comparisons.
Smoking Cessation vs. Nicotine Cessation
Science can not produce even one smoker whose brain reward pathways are chemically dependent upon nicotine-free tobacco. A smoker wouldn't smoke nicotine-free tobacco - containing over 44 deadly carcinogens - any more than they'd roll and smoke dried leaves from the yard. Yet science has engaged in hundreds of NRT studies that compare quitting rates between someone who has quit using nicotine and someone who has not. What have they quit? When did they quit? Is it an honest group comparison?
Do the NRT studies really measure successful cessation or successful transfer of nicotine delivery to a new delivery device? Under such standards, would transferring nicotine delivery from cigarettes to dip, snuff or chew also be considered successful "cessation"? Does science accept responsibility for redefining cessation or was that honor bestowed upon NRT pharmaceutical companies who knew that they'd naturally gain a short term advantage (during two to three months of "therapy", or longer should the quitter become dependent upon their new device) over true quitters, that would allow them to make billions of dollars in profits by calling nicotine medicine, packaging it as therapy and comparing its performance to the real thing - abrupt nicotine cessation? But it appears that even then they were not content to compete against the real thing - it was time to fix the fight.
Placebo Devices Were Doctored
I've had experts tell me that, "the placebo group was given a fair chance." I don't think so! A careful review of the full text of some of the NRT studies relied upon by the U.S. government in making its June 2000 announcement that expensive nico-medicine is now an indispensable part of quitting, reveal that pharmaceutical companies engaged in the practice of lacing placebos with small amounts of nicotine (see Sonderskov, et al., American Journal of Epidemiology 1997 145(4): 309-318, at the top of page 312, where Ciba-Geigy, Inc. supplied placebo patches containing an undisclosed amount of nicotine; Campbell, et al., Respir Med 1996 Jan;90(1):47-51, at page 48, where Ciba-Geigy Ltd supplied placebo patches containing 13% of the nicotine found in the active group; and Ahluwalia JS, et. al., Journal of General Internal Medicine (JGIM) 1998 Vol. 13 (1): 1-8, at page 2, where Marion Merrell Dow provided active patches, and full text indicates that placebos delivered at least 1mg of nicotine every 24 hours).
Why? The lame excuse given is that it was used as a masking agent so that participants wouldn't be able to tell whether or not they were getting the "real thing" at full strength. Have you ever in your life heard of any medical study in which the control group was fed a small amount of the exact same drug being tested by the active group? Why would they be smelling each other's nicotine delivery devices, anyway?
The experts say that, "if anything, nicotine doctored placebos should have helped increase the placebo group's success rate, not decrease it." It sounds good but it's wrong. As any lifetime nicotine user can attest, the "a little is better than nothing at all" theory doesn't work real well for us nicotine addicts.
Nicotine's half-life in the human body is roughly two hours . Within a maximum of 72 hours of ending all nicotine use the brain's dopamine neurotransmitters cease sensing the arrival of any and all nicotine. The user is 100% clean. Amazingly, at the same time, the anxieties surrounding peak withdrawal begin easing off. The basic time trigger - the root catalyst for the creation of all psychological habit feeding triggers - goes unfulfilled and is quickly reconditioned. The abrupt cessation quitter begins to believe that quitting is truly doable at last! Sadly, it's also here, when many sense that quitting might actually be doable and decide to "reward" their hard work with a few powerful puffs of nicotine, that they fail to understand will doom them to defeat.
Not so for those using nicotine spiked placebo delivery devices. Instead, like an alcoholic who keeps taking wee sips, they are artificially held in an unnatural state of serious chronic withdrawal. The 21mg patch user is getting roughly a pack's worth of nicotine a day while the 1 or 2mg of nicotine in the placebo device starves yet refuses to free those using laced placebos. Their choices were three: (1) endure an artificial cessation adjustment experience and the extra time and anxieties needed to become acclimated and comfortable receiving the nicotine equivalent of smoking just one cigarette per day; (2) stop using the device and allow the brain to begin sensing the arrival of nicotine free blood serum; and (3) give-up, relapse, and throw in the towel.
The HONC study findings just released (" Development of symptoms of tobacco dependency in youths." Hooked on Nicotine Checklist , Dr. JR DiFranza, Tob Control 2002 Sep;11(3):228-35) indicate that multiple autonomy loss symptoms of dependency can be established and sensed without using nicotine on a daily basis. If true, the brain is much more attuned to nicotine's presence than those spiking nicotine placebo delivery devices want us to believe. I genuinely believe that placebo nicotine lacing is evidenced by the dismal 4% mid-year placebo group rates showing up in all recent over-the-counter NRT studies. If true, two of the three OTC studies failed to disclose that the placebos had been spiked with nicotine, while the third study disclosed the practice yet failed to reveal the quantity of nicotine used.
Natural Mid-year Cessation Rates
In a series of NRT study review articles that I'll attach links to below, I use the government's own statistical evidence, complied and presented by a panel of volunteer experts with strong financial ties to the NRT pharmaceutical industry , from the USDHHS Clinical Practice Guideline for Treating Tobacco Use and Dependence (June 2000). Their Guideline - which strongly advocates the use of expensive clean-nicotine delivery devices by every quitter on earth, including children, regardless of the amount smoked - presents evidence tables that collectively show that true mid-year on-your-own abrupt nicotine cessation rates are roughly 11%. In other words, the ignorant, untrained, unskilled, and uncounseled cold turkey quitter has an 11% chance of remaining quit at mid-year. It's a rather important fact when you consider that none of the NRT groups performed better than 11% in any of the OTC nicotine patch studies conducted to date, with the average being about two points less at 9%.
How do pharmaceutical company experts explain OTC's dismal performance? Well, their first defense is that it was still twice as "effective" as the dismal 4% rate which is 7 points less than historical on-your-own rates and highly suspect of having been generated by using nicotine doctored placebos (i.e. - 1997 Sonderskov admitted placebo doctoring and generated a 4.2% mid-year rate for 21 mg OTC patch users, while no placebo doctoring was declared in the 1998 Davidson OTC patch study which generated a 4.0% mid-year placebo rate or the 1999 Hays OTC patch study which generated a 4.3% mid-year placebo rate).
If you're like me, once you begin sending emails to pharmaceutical companies asking about doctored study placebos you will not receive any replies. Should you get the opportunity to communicate with the lead authority on a study and ask if there was any nicotine in their placebo devices you're likely to learn that they simply accepted and used the placebo device provided by the pharmaceutical company without ever asking about its contents. If you write the FDA and ask them about it they'll side-step the issue by trying to convince you that quitting is harder today than it was five to ten years ago. The pharmaceuticals may tell you that they've already helped all of the less addicted quitters quit and that those who remain are the hard core addicts. Hogwash!
Just more rubbish! Take your own poll among successful long term quitters. Where are the successful one year NRT quitters? They're not only rare in California but rare in the rest of the world. If you do find one you'll often discover that they abruptly stopped "therapy" eight to ten weeks before recommended. As for quitting being harder, bupropion and other recent non-NRT studies are still generating control group or placebo group rates in the 11% mid-year range ( 13.7% ).
The Tonnesen Recycling Coverup
An earlier clue that NRT can lose any edge it once claimed was buried with a 1993 study by Tonnesen, et. al. entitled "Recycling with Nicotine Patches in Smoking Cessation," published in Addiction, 1993, Apr; 88 (4); at pages 533-539. This early patch study not only substantiates an 11% "on-your-own" rate, it raises an alarming concern regarding "recycling" - the use of NRT for a second or subsequent NRT cessation attempt. One of the factors that the Tonnesen study attempted to determine was how failed patch users from a patch study conducted one year earlier would perform during a second patch attempt. As the study summary (abstract) puts it "all of the subjects had relapsed in the group previously treated with the active nicotine patch." All of them - 100%.
As far as I can tell the neo-nicotine pushers never followed up on the Tonnesen study. I wonder why? I wrote the FDA requesting any study authority contrary to Tonnesen. They replied but produced none. I've asked them to please advise those purchasing NRT for a second time that their chances of success are not 11% but ZERO. To date, my concern has been ignored. I've since learned that the NRT industry has tremendous influence over the FDA, CDC, and entire U.S. Health Department. I worry that their tremendous power and influence is about to come to bear upon Pierce and Gilpin. The NRT industry will feel a need to deter other scientists from ever again questioning their bought and paid for national NRT policy. Sadly, they now have their influence claws into almost every public health organization on earth. These guys are good!
Once acclaimed tobacco control organizations are beginning to appear to be little more than nicotine street pushers for nicotine's new kingpin, the pharmaceutical company. Like the lazy government health bureaucrats who allowed pharmaceutical industry "experts" to write U.S. cessation policy, their blind ambition to destroy the tobacco industry has them in bed with tobacco's only true competitor, clean-nicotine. Their reaction to clean-nicotine being marketed by pharmacists as cessation aids - flavored suckers - has been somewhat two-faced. Although sugar and nicotine is a recipe for accelerated youth dependency, stupid distinctions between nicotine in orange flavored chewing gum and nicotine in orange flavored suckers makes them appear as nothing more than pharmaceutical industry store fronts. Nicotine is nicotine. Imagine teaching children that pure heroin is both a life saving medicine and a deadly killer, depending upon who is selling it.
Where Do We Go From Here?
Clean nicotine is not a panacea or even safe for that matter. Can nicotine in the nicotine patch or gum actually "promote" lung cancer in someone who has never smoked a single cigarette in their entire life (National Cancer Institute's explanation of "promote")? Does nicotine accelerate tumor growth rates for other cancers in the body ( a second link )? Does nicotine cause hardening of the arteries ? Could nicotine be responsible for causing chronic depression ? Does nicotine alone destroy brain cells, learning and memory? If so, why are there no health warnings on the NRT packages?
As Dr. Mark C. Taylor encourages, we need to reflect now upon where ANDS ( Alternative Nicotine Delivery Systems ) is taking us, as that is exactly the direction that these failed NRT marketing campaigns will be forced to turn next. Will the next generation of nicotine dependent youth become enslaved by 27 flavors of nicotine suckers, nicotine water, nicotine soda, and nicotine straws. If you think things are confusing now, just wait until that first child raises their hand and asks you to explain how orange flavored nicotine gum is medicine and therapy, but an orange flavored nicotine sucker is a highly addictive and dangerous product.
It's my hope that the Pierce and Gilpin JAMA article will motivate other scientists around the world to begin taking a much closer look at the massive pile of NRT study data that has already been generated. If they'll turn their focus from the few in the NRT groups who succeeded, to the issues of "when" and "why" those in the placebo groups relapsed, they'll quickly notice a rather consistent pattern. They'll see that the placebo group was slaughtered within the first week. They'll also discover that the small surviving percentage who did navigate early withdrawal went on to outperform the NRT group, from that point forward, in every NRT study presenting one week relapse data.
The key to effective cessation isn't in these newest revelations that eventually the performance of the two groups will meet somewhere down the road (even for Zyban/Wellbutrin/bupropion ). It's in realizing that high quality programs offering participants a solid dependency/cessation education, skills development (on focus, patience and coping), counseling, group support, and reinforcement follow-up (the important factors outlined in Recommendations 5 and 6 of the June 2000 USDHHS Clinical Practice Guideline) have the potential -- like a wonderful tool -- to bring massive numbers of quitters through those first two weeks so that they can stand on firm ground and sense that breaking free is at last entirely within their grasp!
We don't begin learning and adjusting to living without nicotine until we're willing to give it up. Nicotine is not medicine and quitters playing with it, even when supervised, are not engaged in "therapy." Eventually their brain would be required to learn to live and become comfortable with natural levels of dopamine and adrenaline production. That temporary period of chemical and psychological adjustment called quitting can never truly begin until the heart stops pumping nicotine into the brain.
They sold us on the belief that nicotine gum would allow us to break our psychological habit trigger links associated with the times, places, locations, events, emotions and cues that we'd each selected as regular nicotine feeding times. In part it was true, but all the OTC studies provide compelling evidence that the manner or time of feeding isn't nearly as important as the act itself or the sea of memories -- in some cases millions -- created during the feeding process. If trigger reconditioning is a crucial first step toward successful cessation then why did we ever need to invent the concept of NRT in the first place? Why couldn't smokers have just started chewing cheaper nicotine filled chewing tobacco instead of expensive nicotine laced gum? Why couldn't those addicted to chewing tobacco simply take up smoking cigarettes and then gradually wean themselves? Think about it!
It's my hope that science will use the Pierce and Gilpin finding that NRT is ineffective as a wake-up call and opportunity to identify and study those high quality programs that truly are effective. It's my fear that they'll simply make a mad dash to devise the next new quick fix magic cure that teaches nothing while depriving millions of nicotine dependent humans of even more of their limited serious cessation opportunities (once every three years). I fear that two decades of toying with clean-nicotine (NRT) has cost tens of thousand so quitters their lives. If it is later learned that pharmaceutical company executives knew that NRT was ineffective while advertising to the contrary, or that any study was intentionally fixed, or that negative study findings were hidden from view, then thousands of needless deaths have occurred and the heads of all who knew must roll. There must be accountability when it comes to public health!
Not since May 31, 1999, when Dr. Mark C. Taylor, President of Physicians for a Smoke Free Canada published his report entitled " Beyond Pharmaceutical Solutions " has the cessation world been challenged to open its eyes and look around. As in Canada, NRT has been widely available for over two decades, tobacco is killing off U.S. smokers at the rate of 450,000 a year, yet today we have as many smokers in the U.S. as we had a decade ago. Where's the beef, NRT? If science will only explore and study the detail associated with those high quality programs already in existence - that today consistently generate 40 to 50% one year cessation rates -- they could define, refine and supplement what works while raising the bar to unheard of heights. At the risk of sounding skeptical, only time will tell which patch - I mean path - they'll choose.
JAMA Study Publication Date of 9/11
In a sick sort of way it almost seems appropriate that this very important study was published in JAMA on the very day when America remembers the 2,823 victims of the WTC attacks. Not to in any way diminish the significance of the wonderful lives lost on 9/11, the United Nations says that today tobacco will claim 10,958 lives. It will kill the same tomorrow, and the next day, and the next, and the next, as far as the calendar turns. Yes, the difference clearly is that tobacco's victims were warned of the harms and each had a chance to quit. But still, over 90% of them became chemically addicted to nicotine while teenagers, few had advance warning of nicotine's power to quickly and permanently enslave the brain's reward pathways, and precious quit attempts are being squandered by greed and ignorance driven organizations that sadly continue to advocate and push clean-nicotine down the throats of humans dependent upon nicotine.
Is death the proper punishment for what they thought would be just another brief rebellious experiment as children, a childish attempt to look more adult, or believing the tobacco company ads that smoking would make them cool and accepted by their peers? Where is the outrage over their death? Why aren't we going to war? Where are the world's tears? An entire new generation is now being coaxed into experimenting with nicotine. They're just 12, 13, 14, and 15. Sadly, many have yet to even once be told the truth about nicotine's tremendous power. Is a lifetime of enslavement, and a 50/50 chance of dying over 5,000 days early, proper punishment for them as well?
A Message to Long Term NRT Users
All hooked on the cure are invited to visit Turkeyville, WhyQuit's 13,000+ member Facebook cold turkey support group. Your freedom and lives are just as important as any of ours! There are few among us who didn't either begin this quit or prior quits by playing with clean-nicotine. Yes, we measure quitting differently that you've been doing (no nicotine) but don't feel alone or betrayed. We all wanted to believe in a cure. It has long been my belief that the few who were disciplined enough to endure gradually weaning themselves from nicotine were the strongest of all and had the ability all along to put all nicotine aside. I tried four times - 2 gum quits and 2 patch quits - and I wasn't one of the strong. Thank God I didn't need to be! It's time to put the nicotine away. It's time to go to quitting school. Knowledge is power!
I, John R. Polito, am 100% solely responsible for the content of this article and assume full responsibility for its internet publication. It had not been reviewed by any other person prior its internet publication on September 11, 2002, nor had any other person had any input upon its content. The views expressed here are my own, in my individual capacity, as a concerned nicotine cessation and control advocate.

{kind=link}