Tolerance
Why do I gradually keep needing to smoke, vape, dip or chew more and more nicotine?
As if nicotine taking our dopamine pathways captive wasn't enough, imagine the brain physically needing and requiring more nicotine over time.
Definitions of tolerance include:
1. Decreased responsiveness to a stimulus, especially over a period of continued exposure
2. Diminution in the response to a drug after prolonged use, or
3. Physiological resistance to a poison.[1]
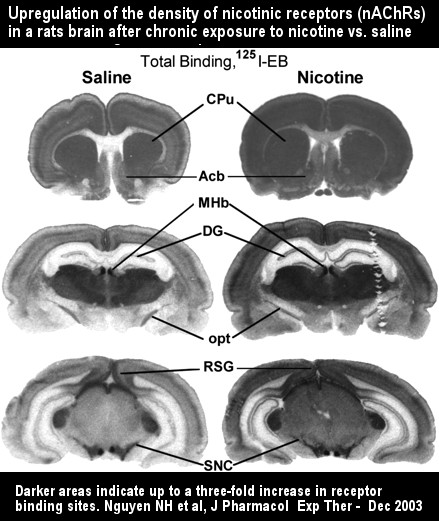
The brain attempts to fight back against its toxic intruder. As if somehow knowing that too much unearned dopamine is flowing, it attempts to diminish nicotine's influence by more widely disbursing it. It does so by growing or activating millions of extra nicotinic type acetylcholine receptors in as many as eleven different brain regions.[2]
Although you'll generally see the average nicotine intake per cigarette stated as being about 1mg (milligram), in truth it varies significantly. For example, the average intake is 30% greater in African Americans at 1.41 milligrams of nicotine per cigarette, as compared to 1.09 milligrams in Caucasians.
Although often stated that the average user's body depletes and eliminates (metabolizes) nicotine at the rate of roughly one-half every two hours, there's variation there too. For example, nicotine's elimination half-life is 129 minutes in Caucasians and 134 minutes in African Americans.[3]
Tolerance ever so gradually pulls us deeper and deeper into dependency's forest. While nicotine's elimination half-life remains fixed, over time we gradually find ourselves sucking a wee bit harder, holding the smoke a bit longer, or using more nicotine in order to avoid wanting or achieve relief from it.
Two a day, three, four, four smoked hard, our brain gradually grew additional nicotinic-type acetylcholine receptors. Over the years, we gradually required a bit more nicotine to maintain our sense of nicotine-normal.
My "aaah" relief sensations were no more powerful smoking five cigarettes a day at age fifteen than when smoking sixty per day at age forty. I needed that much more to keep pace with wanting.
I know, you're probably thinking, you've been at the same nicotine intake level for some time now and it's likely vastly less than the three packs-a-day I was smoking. While we don't yet fully understand wide variations in levels of nicotine use, we know that genetics probably explains most differences.[4]
There is also the fact that some of our mothers, like mine, smoked during pregnancy. I was born with a brain already wired for nicotine. I came into this world as nicotine's slave and likely spent my first few days in withdrawal.[5]
For me, those first few cigarettes at age 15 were not about initial addiction. They were about relapse to a condition that my brain had known since formation and creation of my very first acetylcholine receptor. That first receptor almost immediately became occupied by nicotine that was smoked by mom.
It was an event that occurred three to four weeks following conception.[6] The problem is that receptors are being activated before formation of the brain cell to which the receptor will eventually be attached.
As Duke University Professor Slotkin puts it, "nicotine alters the developmental trajectory of acetylcholine systems in the immature brain, with vulnerability extending from fetal stages through adolescence."[7]
In addition to genetics and prenatal nicotine exposure, the younger we were when we started using, the more profound the altered development trajectory experienced by our still-developing brain.
Research suggests that nicotine inflicted damage to dopamine and serotonin pathways is significantly greater in males than females, but that this female advantage disappears if the female brain is exposed to both prenatal and adolescent nicotine.[8]
The dependent mind is capable of using a low level of nicotine tolerance as justification for continued chemical servitude.
It's easy for those who use less often to rationalize that they are somehow superior or better able to control their addiction than heavy users. In reality, they're hooked solid too. Their slavery is just as permanent and just as real.
The smoker smoking five times a day may also face health risks as great or greater than heavier smokers. This too may be due to genetic factors, to differing toxin and cancer-causing chemical levels found in different brands of tobacco, or to how intensely each cigarette was smoked.
It may also be due in part to environmental factors that subject us to other chemical agents such as radon, or to employment or hobby chemical exposures, or due to the quality of the water we drink and the air we breathe.
Over the years I've met many smokers, myself included, who experienced a significant increase in the number of cigarettes smoked and higher nicotine tolerance following relapse after a failed attempt.
Why? We don't know. Smoking more cigarettes harder, it was almost like binge-eating after dieting, as if my brain was trying to make up for missed nicotine feedings. But seeing increases in the level of smoking following relapse is becoming less common.
Like a hurricane requiring warm water to strengthen, the fuel for a nicotine tolerance increase is additional time and opportunities to use.
The smoke-free indoor-air movement is gradually sweeping the globe. Smoking is also increasingly being prohibited in and around parks, playgrounds, beaches, hospitals, schools and college campuses, and in the presence of children.
Smokers face fewer replenishment opportunities as non-smokers become increasingly less tolerant of smoking in their presence, homes or vehicles. I suspect that the smoker's nicotine tolerance level will increasingly be associated with trying to obtain more nicotine by smoking fewer cigarettes harder.
But the opposite is often seen in smokers transferring their dependency to e-cigs, oral tobacco, or NRT products, where around-the-clock use becomes possible.
"I started out with about 6 pieces a day and now chew about 15 pieces of 2mg per day. Probably more nicotine than when I smoked," asserts a 48 year-old, three-year female gum user.
"There is one in my mouth 24 hours a day, 7 days a week ... yes for real," claims a 32-year-old, three-year male gum user who chews 40-50 pieces a day and thinks he may "chew more than anyone in the world."[9]
Regardless of method of delivery or level of nicotine tolerance, the millions of extra acetylcholine receptors grown by the addicted brain desensitized it to its own natural sense of neuro-chemical normal.
We became wired to function with a precise amount of nicotine in our bloodstream. Not too much, not too little, we worked to maintain and remain within our zone of nicotine-normal. Any attempt to stop using brought potential for a brief emotional train wreck, as we found ourselves not only desensitized to nicotine but briefly to life as well.
"Dependent human smokers have decreased dopamine activity during withdrawal" and withdrawal is accompanied by "a decrease in tonic dopamine activity."[10]
But the brain makes substantial progress in reversing tolerance-induced de-sensitivities within 72 hours of ending all nicotine use. It's primarily a matter of patience, as withdrawal anxieties peak within three days, putting the worst behind us.
Within three weeks the brain will restore the number of receptors to levels seen in non-smokers. Although feeling physically normal again, nicotine's tolerance wiring paths have been permanently burned and etched into our brains.
Although we can arrest our chemical dependency we cannot cure, eliminate, or destroy it. We each remain wired for relapse for life.
While this may sound like a curse, it can become our greatest peace of mind. Once confident of victory, this time we know exactly what it takes to both stay free and fail.
But arrival here on Easy Street involves more than simply arresting a chemical need and level of tolerance.
Use Conditioning
The term "addiction" is generally viewed as being broader than "dependency." Among other factors, it includes the consequences of years of nicotine feedings that involved replenishment patterns and habits that did not go unnoticed by our subconscious mind.
Use habits were fathered by endless compliance with our brain's chemical dependence upon nicotine. Although covered in detail in Chapter 11 (Subconscious Recovery), a basic understanding of nicotine addiction must include mention of use conditioning.
Our subconscious mind became conditioned to associate various activities, locations, times, people, events, and emotions with using nicotine. It learned to expect arrival of a new supply when specific situations or circumstances occurred.
Insula routed urges, craves and anxieties alerted us when conditioned use cues were encountered. Normally the bell ringing use cue and urge was so subtle that it went unnoticed. Almost as if on autopilot, we'd reach for nicotine to satisfy it nonetheless.
You've likely heard of Pavlov, who actually used the ringing of a bell to induce classical conditioning in dogs. He conditioned them to expect food upon hearing a bell. The dogs would actually begin salivating when he rang the bell, even as he started to delay food's arrival longer and longer.
Your unique use patterns conditioned your subconscious too. Encountering a nicotine feeding cue can trigger a response ranging from a barely noticed urge to a full-blown anxiety episode, depending upon your tonic dopamine level.
Teased by thousands of old wanting satisfaction memories, if allowed, the anxiety episode can become emotionally inflamed.
Self-induced anxieties and fears can build, eventually triggering the body's fight or flight panic response. It happens when stress associated with a need, conditioning or desire escalates to the point of registering as a threatening event within the deep inner primitive.
During panic, normal cessation time distortion is made worse, as time seemingly stands still. It can make a three minute crave episode feel like three hours, and entirely unmanageable.
Contrary to what is then felt, those three minutes are extremely short-lived in comparison to active dependency's never-ending cycle of want, urge, use, and satisfy.
Nicotine addiction is about living false priorities, needless conditioning, dishonest use justifications, and denial of all of the above. It's about use of a tiny molecule called nicotine becoming the most frequent lesson taught by a hijacked survival instincts teacher.
Think about it. While we might forget to take our vitamin or medicine, procrastinate regarding work, skip meals, interrupt quality time with family or friends, how often would we fail to respond to the bell for that next mandatory nicotine feeding?
References
- 1. tolerance. (n.d.). The American Heritage Stedman's Medical Dictionary. Retrieved September 14, 2008, from Dictionary.com website: http://dictionary.reference.com/browse/tolerance
- 2. Mugnaini M et al, Upregulation of [3H]methyllycaconitine binding sites following continuous infusion of nicotine, without changes of alpha7 or alpha6 subunit mRNA: an autoradiography and in situ hybridization study in rat brain, The European Journal of Neuroscience, November 2002, Volume 16, Pages 1633-1646.
- 3. Perez-Stable EJ et al, Nicotine metabolism and intake in black and white smokers, Journal of the American Medical Association, July 1998, Volume 280(2), Pages 152-156.
- 4. Berrettini W, et al, Alpha-5/alpha-3 nicotinic receptor subunit alleles increase risk for heavy smoking, Molecular Psychiatry, April 2008, Volume 13(4), Pages 368-373.
- 5. Law KL, et al, Smoking during pregnancy and newborn neurobehavior, Pediatrics, June 2003, Volume 111(6 Pt 1): Pages 1318-1323.
- 6. Slotkin TA, If nicotine is a developmental neurotoxicant in animal studies, dare we recommend nicotine replacement therapy in pregnant women and adolescents? Neurotoxicology and Teratology, January 2008, Volume 30, Issue 1, Pages 1-19.
- 7. Slotkin TA, et al, Adolescent nicotine treatment changes the response of acetylcholine systems to subsequent nicotine administration in adulthood, Brain Research Bulletin, May 15, 2008, Volume 76 (1-2), Pages 152-165.
- 8. Jacobsen LK, et al, Gender-specific effects of prenatal and adolescent exposure to tobacco smoke on auditory and visual attention, Neuropsychopharmacology, December 2007, Volume 32(12); Pages 2453-2464.
- 9. Polito JR, Long-Term Nicorette Gum Users Losing Hair and Teeth, WhyQuit.com, December 1, 2008.
- 10. Grieder TE et al, Phasic D1 and Tonic D2 dopamine receptor signaling double dissociate the motivational effects of acute nicotine and chronic nicotine withdrawal, Proceedings of the National Academy of Science U S A. 2012 Feb 21:109(8); pages 3101-3106. Epub 2012 Jan 20.