
Ex-smokers antithesis of England’s 'don’t
quit cold turkey' Stoptober campaign
Why would any rational government discourage and attack its nation’s most productive and effective stop smoking method?
Although a September 20, 2018 Public Health England (PHE) "Stoptober" press release claims that cold turkey is the "least effective method," comments to a BBC news story reviewing the release overwhelmingly proclaim otherwise.
A quitting method magnet, 86 of 216 comments to the September 20 BBC Health News article entitled "'Don’t Go Cold Turkey' to quit smoking" indicate the stop smoking method successfully used.
 The winner? An eye-popping 77% (66 of 86) stopped smoking cold turkey (CT). Other methods mentioned include 7% who transferred to e-cigarettes, 7% who ingested replacement nicotine (NRT), 6% who engaged in nicotine weaning schemes, 1% who took Champix (Chantix in the U.S.), 1% who underwent acupuncture, and 1% who credited NHS Stop Smoking Services (NHS SSS).
The winner? An eye-popping 77% (66 of 86) stopped smoking cold turkey (CT). Other methods mentioned include 7% who transferred to e-cigarettes, 7% who ingested replacement nicotine (NRT), 6% who engaged in nicotine weaning schemes, 1% who took Champix (Chantix in the U.S.), 1% who underwent acupuncture, and 1% who credited NHS Stop Smoking Services (NHS SSS).
While totally unscientific, the BBC comments are fairly reflective of a growing body of real-world quitting method findings.
A 2013 U.S. Gallup Poll found that more smokers successfully quit cold turkey than by all other methods combined. Among the runners-up, 6% ingested NRT, 2% took prescription pills, and 2% used cut-down methods. E-cigarettes were as yet too new to register.
A 2006 Australian study examined patient smoking and quitting data of 1,000 family practice physicians. CT was the most effective method, doubling the success rate of nicotine gum, patch and inhaler quitters. As for productivity, CT accounted for a jaw-dropping 1,942 of the study’s 2,207 ex-smokers (88 percent).
England’s "least effective method"? Clearly PHE knows that effectiveness relates to real-world performance, while efficacy reflects randomized clinical trial outcomes. Is Public Health England intentionally lying to UK smokers, mistaken, does it not know the difference between effectiveness and efficacy, or is there some other explanation?
PHE and NHS leadership would be well advised to stop listening to paid pharmaceutical industry consultants, and to all beholden to the consultant's profit-sharing PhD study empire.
Instead, UK health officials should sleep on the effectiveness and productivity findings from the July 2018 PLoS One study entitled "Are electronic nicotine delivery systems helping cigarette smokers quit? Evidence from a prospective cohort study of U.S. adult smokers, 2015–2016."
While the study’s primary focus was obviously e-cigarette use, considering the totality of quitting method data from Table 7, not only did CT generate 5 times more ex-smokers than NRT and medication combined, it was three times as effective as NRT, and 2.6 times as effective as e-cigs.
Making Sense of Diametrically Opposed Findings
In 1973, prior to replacement nicotine, Webster’s defined “cold turkey” as "abrupt complete cessation of the use of an addictive drug either voluntarily or under medical supervision." Today, Merriam-Webster’s online definition is largely unchanged: "abrupt complete cessation of the use of an addictive drug."
So, why does cold turkey demolish real-world competition yet flounder in clinical trials? The obvious answer? It was absent.
Smokers wanting to quit CT don’t join clinical trials dangling free NRT or medicine as study recruiting bait. The only competition between NRT and CT occurs out in the streets.
The not so obvious answer? All evidence to date suggests that it is probably impossible to blind experienced quitters as to the onset of their withdrawal syndrome, as the more quitting attempts they make, the more expert they become at recognizing it.
Thus, more than 200 "double-blind" placebo-controlled NRT, bupropion and varenicline studies were not blind as claimed. I submit that in each and every clinical trial, 3 to 4 times as many placebo group members could have correctly declared their randomized assignment as would have declared wrong, and that they could have done so within 24 to 48 hours of quitting (peak withdrawal).
UK NRT experts have an alternative explanation. They contend that divergent clinical trial efficacy and observational study effectiveness outcomes are due to "confounding by indication," that smokers who struggle to quit seek replacement nicotine more often than those who do not.
Reaching to explain the obvious, while likely a factor, it’s tiny in relation to what works and is producing and what’s not. If anything, confounding by indication aids in explaining why outcomes from clinical trials dangling free nicotine bear zero resemblance to population-level quitting. And those suggesting otherwise have cost smokers dearly.
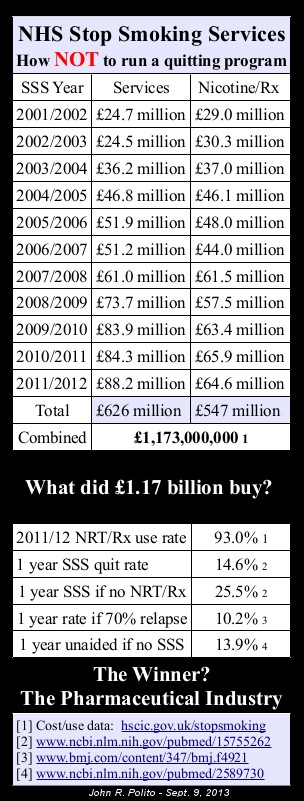
 After decades devoted to junk-cessation-science that was neither blind nor reflective of "your chances," a platoon of UK NRT advocates now watch as NHS Stop Smoking Services (SSS) flounders. The number of smokers setting program quitting dates has fallen for the sixth consecutive year, a 66% decline since 2011/12.
After decades devoted to junk-cessation-science that was neither blind nor reflective of "your chances," a platoon of UK NRT advocates now watch as NHS Stop Smoking Services (SSS) flounders. The number of smokers setting program quitting dates has fallen for the sixth consecutive year, a 66% decline since 2011/12.
The most common reason given for the gradual demise of what’s likely earth’s most expensive government quitting program is the growing popularity of e-cigarettes. But that’s atop 16 years of negative word of mouth associated with 12 of 13 program participants relapsing within a year (2012-13 data); a dismal 92% chemically validated program failure rate.
England Drowning in Nicotine
During 2017-2018, 93 percent of 274,021 NHS SSS quitters were strongly encouraged to use NRT, varenicline (Champix) or bupropion (Zyban), almost the exact opposite of the 2006 Australian Study where CT generated nearly all successful quitters. But how and why?
According to his online curriculum vitae (CV), University College London Professor Robert West is the "Founder and Honorary Co-director of National Centre for Smoking Cessation and Training: responsible for knowledge transfer and evaluation (this organisation was set up by the DH and has trained 16,000+ stop smoking advisors treating some 700,000 smokers per year)."
West's CV also states that he is an "Advisor to English NHS Stop-Smoking Services: continued advice and free consultancxy to the services on a near daily basis with regard to configuration of services, type of behavioural support provided and medication options."
While expressly denying accepting tobacco or e-cigarette industry money, West’s 2018 financial conflicts disclosure openly admits that:
"RW has received travel funds and hospitality from, and undertaken research and consultancy for pharmaceutical companies that manufacture or research products aimed at helping smokers to stop. These products include nicotine replacement therapies, Champix (varenicline) and Zyban (bupropion). This has led to payments to him personally and to his institution."
Stop Smoking Services first received national funding in April 2000. A conflicts disclosure appearing in a paper accepted in May 2000 read, "Robert West has received research and travel funding from, and undertaken consultancy for, manufacturers of nicotine replacement products and other pharmaceutical companies developing products for smoking cessation."
Instead of studying, identifying and incorporating the keys to successful abrupt nicotine cessation into facilitator training and NHS SSS programs, in September 2017 West helped author a PHE report entitled "Models of delivery for stop smoking services." Doubling down on nicotine, it states:
"[E]cigarettes can help smokers to quit, may be at least as effective as licensed medications and that an increasing number of people are choosing this option. Recommendation: Stop smoking services should offer an 'e-cigarette friendly’ approach. This involves being open to the use of e-cigarettes by those who wish to do so, providing behavioural support and offering stop smoking medications alongside an e-cigarette if chosen by the indvidual."
England’s National Institute for Health and Care Excellence (NICE) is the UK’s official public health gatekeeper and guardian of evidence-based guidance, advice and standards, including those for smoking cessation.
In March 2018, NICE issued Guideline NG 92, "Evidence reviews for advice on e-cigarettes on general sale." It recommends that health practitioners explain to smokers interested in using e-cigs that although not licensed medicines, "many people have found them helpful to quit smoking cigarettes."
Although not known whether Professor West helped advise or author NICE's e-cigarette policy change, his online CV states that he is a "Member of NICE Programme Development committees: helped produce guidance on brief advice, behyaviour change, stop-smoking services, and tobacco harm reduction."
On April 26, 2018, University of Sidney Professor Simon Chapman responded to an April 25 British Medical Journal online debate entitled "Should we recommend e-cigarettes to help smokers quit?"
"The English tobacco control/smoking cessation community is internationally regarded as utterly, hopelessly smitten with ecigs," Chapman wrote. "It’s become almost cult-like."
Professor Chapman noted that, "They have long framed smoking as something that needs to be somehow medicated or pharmacologically assisted, whether this be with NRT, prescribed medications, or now ecigarettes, when the awkward fact is that most ex-smokers have always (and still do) quit without any of these methods when they finally succeed."
Citing a 2014 study co-authored by West, Chapman noted that, "The consensus on the 'success' of NRT outside of such professional assistance is now that it is actually lower than unassisted cessation. Eg: ('The use of NRT bought over the counter was associated with a lower odds of abstinence (odds ratio, 0.68; 95% CI, 0.49-0.94')"
Which brings us to PHE’s Stoptober doorstep and its new "Personal Quit Plan" generator on its OneYou website (www.nhs.uk/oneyou/).
As of today (09/28/18), all "personal" plans generated recommend using both e-cigarettes and NRT, with e-cigs getting top billing. This occurs regardless of the smoking and quitting history the smoker selects, including: (1) smoking the least number of cigarettes daily, (2) waiting the longest after waking before smoking, and (3) if never having previously attempted quitting.
Also, as for quitting methods previously used, although the generator tells you to "Pick as many as you like," try claiming that your prior attempts included both "Willpower alone" and any other method. Big pharma must be smiling, as before its eyes willpower gets blamed for all prior defeats.
The online Personal Quit Plan generator provides a visible sampling of how NHS SSS facilitators have been trained to coerce 93% of quitters (see Table 4.4) into betraying their natural quitting instincts. Try test driving the plan generator a second time using alternative personal data. You will need to delete your browser’s cookies before doing so.
What is Professor West’s involvement in PHE’s Stoptober campaign? Again, according to the online CV available on 09/28/18 at http://www.rjwest.co.uk/, he is an "Advisor to Public Health England Communications Team: helped design and establish Stoptober campaign and overall communications strategy since 2008; regular input to communications policy, ongoing collaboration on development and implementation of digital interventions to promote and aid cessation (e.g. StopAdvisor)…"
Is PHE’s Personal Quit Plan generator broken when it comes to either ignoring "willpower" attempts or forcing CT to accept blame for all prior relapses, or is such function purposeful?
Funded by Pfizer and GlaxoSmithKline, Robert West is the creator of the "Smoking In England" website (http://www.smokinginengland.info/). There, what’s glaring about his quitting method survey site is the total absence of England’s most popular and productive quitting method.
Cold turkey is not listed as one of the 16 possible responses to the survey question (Word doc), "Which, if any, of the following did you try to help you stop smoking during the most recent serious quit attempt?" (see pages 14, 18, 22 and sixty additional pages of quitting method questions).
England's undefeated real-world quitting champ since invention of the cigarette-making machine 136 years ago, as evidenced by comments to the Stoptober BBC story, there's no equivocation among UK ex-smokers about identifying as cold turkey quitters.
Why can’t West do the same? Why should the vast majority being interviewed be forced to wade through a long list of named quitting methods before the humiliation of being compelled to select "other"?
It's simple. Imagine a Pfizer, GlaxoSmithKline and Johnson & Johnson sponsored survey (see "Grant Support") being forced to declare cold turkey England’s 2018 quitting champion. In pharma's mind, what’s not asked and not known can’t harm you.
Nicotine addiction is a mental illness, a brain dopamine pathway wanting disorder. PHE’s Personal Quit Plan generator plays and preys upon that disorder by urging all quitters to combine use of both vaped and replacement nicotine.
Although the samples are small, Table 7 of the July 2018 PLoS One study provides data allowing UK smokers to compare cold turkey’s effectiveness to all recommendations made by PHE's Personal Quit Plan generator: to vape nicotine while also using replacement nicotine.
According to Table 7 data, cold turkey is nearly five times as effective as PHE’s recommendation. While 56 of 129 cold turkey quitters were not smoking at follow-up (43.4%), only 5 of 54 who both used NRT and e-cigarettes had quit (9.2%). Even then, what percentage of the 9.2% remained slaves to nicotine?
Being home is vastly more do-able and infinitely more wonderful than the daily grind of living from fix to fix. And the path toward permanently ending wanting, urges and craves for more nicotine is as simple as making and sticking to a personal commitment to never take another puff, dip, vape or chew.
Baby steps, just here and now, these next few moments, yes you can!
I, John R. Polito, am fully and solely responsible for the content of this article. Any factual error will be promptly corrected upon notice emailed to john@whyquit.com

{kind=link}
{kind=link}