
The Surgeon General's Reports: 50 years of cessation ignorance
January 20, 2014 by John R. Polito
Omitted from the curriculum of nearly every medical school, the Surgeon General's Reports have been a missed opportunity to teach critical nicotine dependency recovery lessons, including how nicotine addiction is a brain dopamine pathway wanting disorder that's as real and permanent as alcoholism, that when quitting lapse nearly always equals relapse, the importance of blood sugar stability, that cessation blood caffeine levels double, and that half of relapses are associated with alcohol use.
As for relapse, as Dr. Luther L. Terry, the U.S. Surgeon General who chaired and helped author the landmark 1964 "Smoking and Health" report quickly learned, when it comes to avoiding smoking relapse, an understanding of "why" smokers smoke is critical.
Imagine America's most celebrated physician - the U.S. Surgeon General - being expert at declaring smoking's harms, yet totally ignoring study of how most ex-smokers successfully arrest their addiction.
The Surgeon General - Living His Error
 Like nearly all Surgeon General reports since, the famous 1964 report linking smoking to lung cancer is void of meaningful cessation advice. How could it be otherwise? The brains of half of the advisory committee members were themselves slaves to smoked
nicotine and mentally
ill.
Like nearly all Surgeon General reports since, the famous 1964 report linking smoking to lung cancer is void of meaningful cessation advice. How could it be otherwise? The brains of half of the advisory committee members were themselves slaves to smoked
nicotine and mentally
ill.
Still, their lived health hypocrisy compelled all but one to arrest their chemical dependency soon after the report was released. It would take another year and a lung cancer diagnosis before chain-smoking Harvard chemistry professor Louis Fieser broke free.
According to a 1998 documentary, Surgeon General Terry was smoking a cigarette while reviewing his notes during his ride to the State Department for the January 11, 1964 report press conference. One of his aides said, "you know, they're going to ask you about that." "I know," he replied.
Following the press conference, Dr. Terry called for questions.
"Dr. Terry, do you smoke?" "No sir, I don't," he replied. "Dr. Terry, have you ever smoked?" "Yes, I used to." "Dr. Terry, when did you quit?" "About 10 minutes ago."
Imagine half the panel, including Dr. Terry, then and there struggling to understand and come to terms with who they were: real drug addicts.
What greater evidence of smoked nicotine's addictiveness than being unable to refrain from smoking during meetings while authoring history's most famous report on its devastating consequences?
Blinded yet protected by the exact same dependency denial that today insulates 33 million daily smokers from their slow suicide and gradual self destruction, then and there, even with eyes opened, real drug addiction was too great and personal an admission for Dr. Terry to make.
And it must have been comforting to all advisory committee smokers that the lone pharmacologist, Dr. Maurice H. Seevers, was wrongly convinced that there was no observable physical abstinence syndrome associated with smoking cessation. Thus, by his analysis, it didn't fit drug addiction's accepted definition.
"The overwhelming evidence indicates that smoking - its beginning habituation, and occasional discontinuation - is to a very large extent psychologically and socially determined," page 32 of the first Surgeon General's report declared.
While the report was wrong in identifying the engine of disease and "why" smokers smoke, nearly every report since has been in error as to the engine's key, and "how" to quit.
Although dependence was mentioned in the 1979 Surgeon General report ("an increasing desire or need for the effects"), not until the 1988 report of Surgeon General C. Everette Koop would this addiction physiology error be formally corrected (tobacco is "addicting" and "nicotine is the drug in tobacco that causes addiction").
Lessons Missed
"I was physically and psychologically dependent upon cigarettes and found it easier to suppress my knowledge rather than give them up,"Dr. Terry would write twenty years later in the Forward to "A Smoking Gun."
As he there noted, millions quit following release of the report. "Sales dropped and we were jubilant," recalled Dr. Terry. "We imagined for a moment that we had 'conquered' cigarette smoking. We were wrong. Not altogether wrong but mostly wrong. Within a few months, millions of those who quit had started to smoke again."
"We vastly underestimated the dependency factor involved in cigarette smoking. Our 1964 report had called smoking a 'habit.'" "Today we know that cigarette smoking is compulsive for many if not most smokers. Smoking is unquestionably a form of drug addiction just like heroin use," wrote Dr. Terry in 1984.
Over the past 50 years, 31 Surgeon General's Reports on smoking have been released. While unparalleled in defining the problem and attempting to coerce cessation via fear, they've been worse than worthless in teaching cessation.
Surgeon Generals Hostage to Junk Science
The new January 17, 2014 Surgeon General Report is no exception. It's entitled "The Health Consequences of Smoking - 50 Years of Progress: A Report of the Surgeon General." Once again, the progress has been in identifying the diseases by which smoke cripples and kills.
While it clearly attempts to coerce cessation via fright, another 50 years of risk discoveries cannot undo dependency's physiology nor un-saturate or down-regulate a single a4b2 nicotinic receptor.
As Dr. Terry discovered long ago, while fear is a powerful initial motivator, it lacks staying power, as smokers quickly grow numb to it.
It's a lesson reinforced by graphic cigarette pack health warning photos, which appear to have greater influence upon youth smoking initiation than in motivating successful cessation.
The pharmaceutical industry and its army of financially conflicted quitting product researchers have ground cessation to near standstill. They ask us to wear blinders as to the massive and deadly disconnect between placebo-controlled quitting product efficacy victories and consistent population level effectiveness defeats.
They ask us to pretend that dangling free quitting products in front of smokers in order to induce study participation doesn't induce substantial expectations bias, as smokers with significant quitting histories seek to experience a diminished withdrawal syndrome.
They ask us to pretend that a nicotine addict with a lengthy quitting history hasn't become expert at recognizing onset of their withdrawal syndrome.
They ask us to pretend study blindness as to the onset of full-blown withdrawal when up to 90 percent of study participants had prior quitting histories, when 3-4 times as many placebo group members are able to correctly declare their randomized assignment to placebo as guess wrong, and can do so within 24-48 hours of cessation (peak withdrawal).
They ask us to pretend that ongoing cessation counseling, whose primary initial focus is to foster continued brain dopamine pathway stimulation, with continued receptor up-regulation via successful transfer to NRT, bupropion or varenicline, has equal and fair value to a placebo group participant badly in need of abrupt cessation counseling basics.
Most disturbing, they continue to represent to cold turkey quitters that dismal placebo-group clinical efficacy outcomes, from trials in which those seeking free quitting products, diminished withdrawal, and assigned to a placebo look-a-like instead, reflect "your chances."
Invested far too deeply to turn back, or lacking the courage or economic independence to dare bite the hand that feeds them, many stakeholders will seize upon this new report's list of additional diseases in helping use fear to sell their benefactor's worthless products.
Sadly, the Surgeon General was missing-in-action as the neo-nicotine industry re-labeled the natural insecticide nicotine "medicine," termed its use "therapy," and began conducting apples to oranges studies which compared an addict who had ended brain dopamine pathway chemical stimulation to one who had not.
More than 200 placebo-controlled smoking cessation trials failed to verify that even one participant had fully arrested their addiction to nicotine. No testing of blood, saliva or urine for the absence of nicotine, as with the first Surgeon General's report, we've seen 50 years of ignoring addiction.
Recent Surgeon Generals Absent Without Leave
While population level epidemiology was critical to Dr. Terry's 1964 findings, Surgeon Generals since 1999 have remained silent as pharma's paid consultants were invited to author official U.S. cessation policy in 2000 and again in 2008.
Both times, without challenge, they declared population level cessation findings and outcomes non-science-based, while mandating approved quitting product use by all.
"The great and powerful pharma has spoken!" "Pay no attention to that man behind the curtain!" "From this day forward, all federal and state health officials work for us, and have no choice but to sell and push our nicotine medicine therapy!"
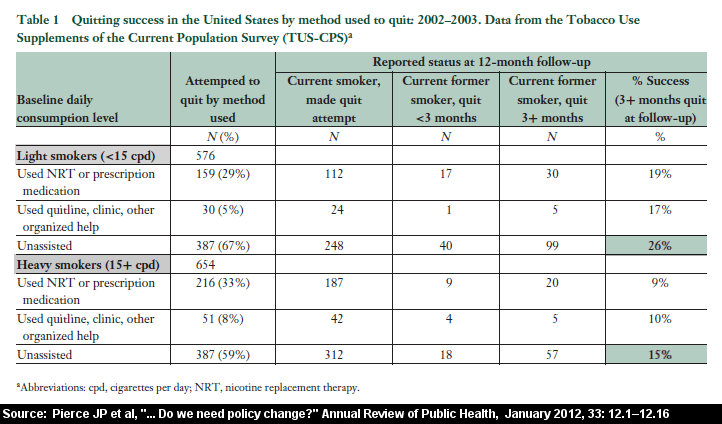
Physicians and government health workers are asked to ignore the fact that, as found by a July 2013 Gallup Poll, more patients quit smoking cold turkey than by all other methods combined, that only a tiny fraction of successful cessation involves use of any approved product (just 8 percent).
Reflect on the fact that after 30 years and billions spent marketing Nicorette, that the Gallup Poll found that only 1 in 100 succeeded via nicotine gum. The quitting tail is not only wagging the dog, its killing it (example: see Neil Curtis' quitting journal).
Fifty years of progress? Survey after survey teaches that feeding nicotine to nicotine addicts has nailed cessation to the floor, and that force-feeding weaning programs are costing lives (see Doran 2006, Hartman 2006, West 2006, Cheong 2007, Ferguson 2009 and Pierce 2012).

Don't expect to find any abrupt nicotine cessation paper cited in the General's 978 page report. None.
Why? Because the 50th Anniversary Surgeon General report invited a number of financially conflicted researchers to help write it. Although impossible to know the role each played, to these eyes, their master's bidding leaps from the report.
The report repeatedly and falsely implies that quitting products work, including replacement nicotine (NRT), and are effective at helping smokers quit, without mention of the large and growing body of real-world findings to the contrary (see messages of Sebelius and Koh, and pages 30, 109, 812, 816 and 820).
It also suggests that NRT has a role in long-term maintenance as a smoking substitute (Page 109, 787 and 854), a move that would put pharma's nicotine on equal economic footing with the e-cig industry's.
The Report primes the NRT and e-cig addiction sales pump by praising nicotine's cognitive stimulant effects (Page 121), while ignoring its neuro-toxic ones, except in regard to the fetus (Page 129). Even there, the report sends mixed signals regarding the appropriateness of NRT use during pregnancy (Page 464).
The report falsely asserts that dependence upon nicotine gum is rare (when up to 6.7% of gum quitters get hooked) and that should it happen that it's substantially easier to quit gum than tobacco (Page 112).
Behaving frighteningly like the nicotine industry prior to 1964, it uses the ambiguous word "development" in giving replacement nicotine the all-clear in "having no appreciable effect on the development of cancer," when a number of studies suggest that nicotine promotes cancer (Page 285).
The Surgeon General has also been used in support of pharma's ongoing war in undermining cold turkey, the method getting the lions share of quitting attempts.
Historically cold turkey has been defined as the "complete and abrupt cessation of a drug." Recognizing the laughability of NRT's contribution to successful cessation, pharma's most recent tactic has been to attempt to redefine the elephant in the room - cold turkey - out of existence.
Last year WhyQuit.com, the Internet's leading cold turkey quit smoking website had 2.2 million unique visitors. Site visitors find gripping motivational stories, hundreds of original cold turkey articles, more than 200 video lessons, two free quitting ebooks ("Never Take Another Puff" and "Freedom from Nicotine - The Journey Home") and are supported by our cold turkey quit smoking support group, Turkeyville.
What's fascinating is that by the new "cold turkey" definition that somehow wormed its way onto page 846 of this 50th anniversary report, no quitter who succeeds by use of the Net's leading cold turkey site is any longer a cold turkey quitter.
According to the Surgeon General's new nonsense definition, quitting "cold turkey" means "quitting without seeking help from a health care provider, program, or other cessation services."
This masking mud is echoed on the newly revised SmokeFree.gov website, where the only reference to the method which generates more successful ex-smokers than all others combined asserts that "Most people who quit don't quit cold turkey on their own." "They get a lot of help and support from friends, family, and significant others."
Enough is Enough!
If the 50th anniversary report is correct, nearly a half a million Americans will be claimed due to addiction to smoked nicotine during 2014. It's time for real health leadership, a Surgeon General like Terry or Koop with the courage to speak truth to power, and admit where we went wrong.
Director of WhyQuit since 1999, on April 27, 2007 I had my oldest daughter reach through a Charleston rally crowd and hand then smoking Senator Obama a copy of my mentor's popular cold turkey quitting book "Never Take Another Puff."
I've since written the White House multiple times. My most recent attempt on October 26, 2013 was an open letter entitled "One nicotine addict to another." And therein lies the problem.
Like Dr. Terry prior to his press conference, my President is currently an actively feeding nicotine addict in full denial. I know he has a lot on his plate, but it was disheartening that he failed to even briefly appear at Saturday's White House unveiling of the anniversary Surgeon General's Report.
I couldn't disagree more with Secretary Sebelius' ceremony assertion that "no President has ever been as committed to ending the epidemic of tobacco related deaths as President Obama."
Sadly, and with deep regret, I must submit that no President in history has done more to ensure that the dying continues unabated.
Philip Morris, America's largest cigarette maker, worked hard to get President Obama to sign the Family Smoking Prevention and Tobacco Control Act. The law granting the U.S. Food and Drug Administration (FDA) jurisdiction over tobacco not only handed the cigarette an official government birth certificate, it instantly transferred culpability for all smoking related deaths to the federal government, while tying the FDA's hands behind its back.
The language of the bill, drafted by Philip Morris, deprives the FDA of the power to ban the sale of cigarettes, smokeless tobacco, little cigarettes, pipe tobacco, roll your own tobacco, or from requiring removal of nicotine from cigarettes. Additionally, it grants the nicotine industry a host of substantive and procedural rights which guarantee a legal quagmire sufficient to block implementation of any FDA plan to diminish dependency, disease or death.
The "Family Smoking Prevention Act" did not force removal of a single cigarette marketing sign from any neighborhood store, millions of which daily encourage teens to smoke and experience wonderful flavors and tremendous pleasure. The Act effectively guarantees their survival.
And who did my President select as director of the FDA's new tobacco office? A senior vice president of the firm having exclusive Nicorette consultancy responsibility: a neo-nicotine salesman. It's the same worthless Nicorette that the President has on occasion been filmed using and promoting to others.
Knowing there was a question and answer session following Saturday's program, why would any Nicorette dependent President risk the grilling Dr. Terry underwent, a frank discussion about his brain dopamine pathway "wanting" disorder?
More than two million nicotine induced deaths since President Obama took office, yet no open war, the Commander in Chief missing in action, and no frank and honest dependency discussions.
Why? Because my President's image is more important than the half million who'll die this year. Because the exact same dependency ignorance and denial Dr. Terry battled in 1964 remains America's #1 killer today.
I, John R. Polito, am solely responsible for the content of this article. Any factual error will be immediately corrected upon receipt of credible authority in support of the writer's contention. E-mail comments to john@whyquit.com

{kind=link}
{kind=link}