FDA quit smoking products again lose to cold turkey
While the Surgeon General acknowledged in January that cold turkey is the real-world quitting champ, government websites continue to say otherwise.
 Through a smoker's eyes, does the phrase "your chances" refer to real-world performance and effectiveness, or clinical efficacy versus placebo?
Through a smoker's eyes, does the phrase "your chances" refer to real-world performance and effectiveness, or clinical efficacy versus placebo?
Despite cold turkey prevailing in nearly all population-level studies, the CDC and its SmokeFree.gov website continue telling smokers that "Quit smoking medications can double your chances of quitting for good."
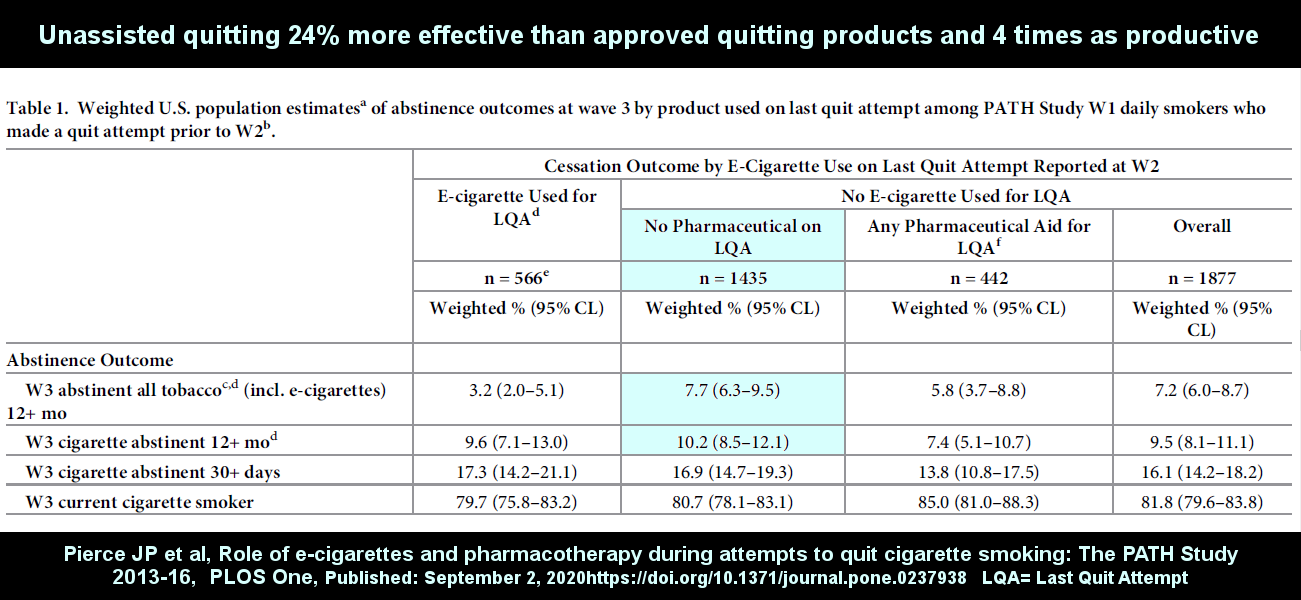
Led by UC San Diego Professor John P. Pierce, on September 3, 2020, the latest salvo, the real-world quitting method findings of 36 prominent cessation researchers, was published online at PLOS One.
According to study Table 1, smokers quitting without the use of any pharmaceutical aid were 24% more likely to be abstinent from all forms of tobacco after 12 months, including e-cigs, than those using FDA approved quitting products.
As for ex-smoker productivity, unassisted quitting produced 4.2 times as many success stories as approved products.
According to the study,"Randomized trials are well suited for demonstrating efficacy, but they do not always translate to the general population."
But why? Why do approved products prevail inside clinical trials yet fail to prevail in real-world use?
As the authors note, "Understanding what leads to the differences between these types of studies is important to optimize the public health potential and ways to deliver these interventions."
Per the PLOS One study, "evidence from NRT studies suggests that discontinuation of a cessation product is often associated with relapse to smoking."
As in nicotine lozenge studies where the treatment period was 6 months, imagine declaring victory while the chemical stimulating the active group’s brain dopamine pathways is still circulating in their bloodstream.
The authors also noted that "the optimal cessation aid package tested in trials is rarely what is implemented at the population level."
Webster defines "bait and switch" as a "ploy of offering a person something desirable to gain favor then thwarting expectations with something less desirable."
Clinical trials nearly always wrapped approved products in weeks or months of counseling or support designed to encourage and motivate successful nicotine weaning via NRT, products and counseling worthless to the study’s placebo arm.
Chantix trials set records for the number of counseling/support contacts (26 times in Jorenby 2006), when, after visiting the doctor and filling their real-world prescription, nearly all Chantix users are totally on their own.
"Further, the selection criteria for randomized trials may limit generalizability to the population."
Clinical trials suffer from extreme selection bias. Ask yourself, how many cold turkey quitters join clinical trials dangling free NRT or medication as study recruiting bait?
"In addition," asserts the Pierce study, "different measurement methods may result in different outcomes between randomized trials and population-based studies."
Clinical trials compared apples to oranges. Reflect on the logic of equating and measuring the accomplishment of an alcoholic who quit drinking to one who simply transferred to a new form of delivery.
Nearly all clinical trials involved the use of placebo controls. While normally the clinical-trial gold standard, since the very first nicotine gum studies, smoking cessation trials have been plagued by an inability to blind experienced quitters as to withdrawal’s arrival.
The Pierce study’s primary objective was to determine whether e-cigarettes were effective in helping population-level smokers quit. Did e-cigs prevail? No.
Again, according to Table 1, when quitting is defined as ending the use of all tobacco products, including e-cigs, unassisted quitting was twice as effective at helping smokers arrest their dependence upon nicotine after 12+ months.
What about productivity, the number of successful ex-smokers generated? Eight times as many unassisted smokers quit smoking as did e-cig users.
After 12+ months 18 of 566 e-cigarette users had succeeded in quitting smoking (9.6%) compared to 146 of 1,435 (10.2%) who quit cold turkey.
Even then, as noted by the study, "Over half of those who used e-cigarettes to try to quit were still using e-cigarettes."
So long as SmokeFree.gov is encouraging tweeting of the message "You have options. Quitting 'cold turkey' isn’t your only choice, and choosing another option can improve your chances of success," findings such as those in Pierce 2020 will remain hidden.
And then there are SmokeFree.gov quitting booklets such as "Clearing the Air," where page 10 tells smokers that "For some smokers, 'going cold turkey' seems like the easiest way to quit: Just stop smoking and tell yourself you’ll never light up again. This works for some smokers -- usually those with the lowest level of nicotine dependence -- but not many. Fewer than 5 percent of smokers can quit this way ... Research shows that most smokers have more success with one of the assisted quit methods discussed below."
Sadly, the longer that SmokeFree.gov continues claiming that approved products "double your chances," the longer cold turkey quitters exploring the site will leave discouraged and demoralized, relapse, and risk becoming a smoking statistic.

{kind=link}
