
Surgeon General: most smokers succeed cold turkey
February 13, 2020 John R. Polito
New report notes evidence that cold turkey may be superior to NRT

How do most smokers successfully quit? It's the most fundamental quitting question of all. What method did they use?
Government health officials have had a conflict in sharing an honest answer to that question since January 13, 1984, the day Nicorette finagled FDA approval.
The conflict's pinnacle occurred in June 2000, when an 18 member panel that included 11 paid pharmaceutical industry consultants was allowed to author official U.S. quitting policy. Their USDHHS stamped policy document was titled "Treating Tobacco Use and Dependence: Clinical Practice Guideline."
Chicanery in pretending that real-world effectiveness mirrors clinical efficacy, the 2000 Guideline parroted Glaxo Wellcome's 1997 million dollar endowment (created for the soon to be Guideline panel's chairman) in decreeing that:
"Numerous effective pharmacotherapies for smoking cessation now exist. Except in the presence of contraindications, these should be used with all patients attempting to quit smoking."
Twenty-five words and pharma had won.
U.S. policy remained firmly under pharma financial influence on May 7, 2008, when many of the same conflicted experts were allowed to author a "Guideline Update" adding Pfizer's Chantix (varenicline).
At Last, The Truth
"Smoking Cessation: A Report of the Surgeon General" was released on January 23, 2020. Millions of deaths slower than China's sudden change of heart in telling the truth about existence and spread of the coronavirus, the Report raises the prospect that when it comes to successful quitting, that cold turkey has always been king.
Under the heading "Perspectives on Smoking Cessation," Page 15 of the Report states:
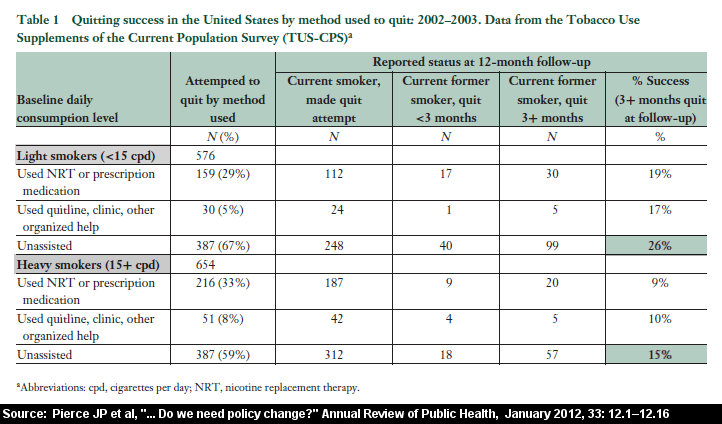
Proponents of encouraging smokers to quit without treatment, often called quitting "cold turkey," point to data indicating that most smokers who quit successfully do so without medications or any type of formal assistance, as well as to population surveys suggesting that cold-turkey quitters do as well or better than those who use over-the-counter NRTs. Proponents of this approach also suggest that medicalization may disempower smokers and create artificial barriers to quitting (Alpert et al. 2013; Polito 2013).
Frankly, it's exhilarating witnessing nearly two decades of government suppression of quitting's most fundamental question, hopefully, come to an end.
It's also a tad bizarre having my free quitting ebook cited by the Surgeon General as a primary source questioning the sanity of declaring the toxin nicotine medicinal and its use therapy (footnoted on Report page 30 as: Polito JR. Freedom from Nicotine: The Journey Home, 2013; https://whyquit.com/ffn/index.html; accessed: September 14, 2017).
Still, while a single paragraph of the Report proclaims how most succeed, and that CT may be superior to OTC NRT, the other 699 pages read as though quitting's production champ is nonexistent.
What are the keys to successful cold turkey quitting? Can they be easily shared? And shouldn't those be burning questions inside the mind of the Surgeon General and every credible cessation researcher?
Another brief mention of cold turkey occurs on Page 95, where the Surgeon General demonstrates that kids may understand the definition of "cold turkey" better than the Report's authors.
There, after mentioning that the vast majority of high school students had tried to quit unassisted or cold turkey, the Report states:
"However, caution is warranted in interpreting these results because a large proportion of middle school students reported using both a strategy to quit and quitting cold turkey, suggesting that they had different interpretations of what was meant by ‘quitting on their own' or quitting cold turkey."
In 1973, Merriam-Webster's defined "cold turkey" as "abrupt complete cessation of the use of an addictive drug either voluntary or under medical supervision."
Pharma's share of successful quitters is so small that its primary tactic in making it appear larger is to pluck and dismember the giant turkey in the room.
It does so by sponsoring or influencing quitting method surveys that never once ask about cold turkey quitting, surveys that rob cold turkey of all quitters who supplemented their quit with education, support or a supervised "strategy."
Try telling the 13,000 schooled and counseled cold turkey quitters at Facebook's Turkeyville support group that they didn't quit cold turkey, or the millions reading cold turkey quitting books, or receiving abrupt nicotine cessation encouragement and support from their doctors.
Policy Change or Abberation?
Does the Surgeon General's cessation truth-telling reflect a weakening of pharma's 24-year death grip on national cessation policy or a momentary lapse of editorial control?
The balance of the report suggests the latter. After noting cold turkey's real-world productivity and effectiveness, Page 15 of the Report goes on to list four possible reasons why population-level findings may not be reliable.
Those reasons include: (1) financial barriers to obtaining quitting products, including a lack of insurance coverage, (2) selection bias in more heavily addicted and less likely to succeed quitters gravitating toward FDA approved products, (3) improper quitting product use, almost always without counseling, and (4) poor recall as to how - at last – the smoker successfully quit.
Cost: The unit price of a Walmart 24-hour 21mg. Equate nicotine patch is $1.86 nationwide, while in most states Walmart's cheapest pack of cigarettes is $5 or more.
Selection Bias: Most heavy and older smokers succeed without quitting products. Quitting product industry shotgun marketing does not discriminate based upon the viewer's level of dependence. If not, why should population-level cold turkey findings need or require "adjustment"?
Talk about selection bias, how generalizable are findings from more than 200 randomized trials that dangled free quitting products as study recruiting bait, studies effectively discouraging participation by smokers dreaming of quitting cold?
Improper Product Use/No Counseling: The 2018 Weaver study found cold turkey twice as effective as prescription products (Chantix and Zyban combined), and three times as effective as NRT. Imagine the Surgeon General arguing that cold turkey rates would be higher if not for improper cold turkey quitting (see "Joel's Library"), or attempting abrupt cessation without counseling or support?
Recall Bias: Criticized in 2012, this argument stems from the fact that the bulk of failed cold turkey attempts occur within the first week, while quitters using dopamine stimulation products experience higher rates of delayed relapse. Showing up in survey findings, pharma seized upon relapse timing in suggesting that the cold turkey quitter's memory of one of the greatest accomplishments in their life should not be trusted.
Cold Turkey Research Neglect
The report mentions e-cigarattes 20 times more frequently than cold turkey. Reflect on the logic of nicotine dependency transfer (with high dual use rates) getting vastly more analysis, and infinitely more research than successful nicotine dependency recovery.
Why? There is no money to be made from free quitting.
What's needed is research into the key or keys to successful abrupt nicotine cessation, widespread sharing of those keys, and studies pitting smokers schooled in cold turkey basics against quitters schooled in proper use of approved quitting products.
What’s needed are additional studies like Weaver 2018 and Doran 2006, studies examining the entire spectrum of grassroots quitting.
Population-level quitting method surveys need to add an additional question: During your most recent quit attempt, did you quit cold turkey by abruptly and completely ending use of all nicotine products?
Nicotine itself harmful and dangerous, shouldn't nicotine dependency recovery be public health's highest priority, and the benchmark of every cessation study? If so, shouldn't testing body fluids for cotinine (a major nicotine metabolite) become standard at long-term follow-up?
Finally, the Surgeon General's report fails to mention the blinding nightmare that I submit has compromised all placebo-controlled smoking cessation trials. At a minimum, shouldn't it be mandatory for all future placebo-controlled trials to conduct the blinding integrity assessment outlined in Mooney 2004:
"To determine the prevalence of failure, clinical trials of NRT should uniformly test the integrity of study blinds. Moreover, if blindness failure is observed, subsequent efforts should be made to determine if blindness failure is related to study outcome and, if so, to provide an estimate of treatment outcome adjusted for blindness bias. Without these methods and analyses, the validity of NRT clinical trial results could be questioned."
The new Surgeon General's Report cracks the "effectiveness" door. A billion at-risk lives need it to open far wider.
John R. Polito
Nicotine Cessation Educator
Related reading & videos
|
2020 Surgeon General's Report on Smoking Cessation Joel Spitzer video Whatever you do don’t quit smoking cold turkey! Joel Spitzer video page Gallup Poll: Most quitters credit cold turkey Joel Spitzer video How to quit smoking Joel Spitzer video Can you spare about an hour and a half to help to save your life? Joel Spitzer video page Relapse prevention resources Joel Spitzer video Talk to your doctor about quitting smoking Joel Spitzer video Are doctors taught about nicotine recovery? Joel Spitzer video Resources for doctors to help their patients Joel Spitzer video Where can I get information on how to quit smoking cold turkey? Joel Spitzer video |

{kind=link}