
Cytisinicline stop smoking rate quintuples placebo?

Demonstrating 5 times greater stop smoking efficacy than placebo from weeks 9-24 (odds ratio=5.3), the latest Food & Drug Administration (FDA) phase 3 drug approval victory for 3mg. of the natural alkaloid cytisinicline (cytisine) taken 3 times daily for 12 weeks was off the charts.
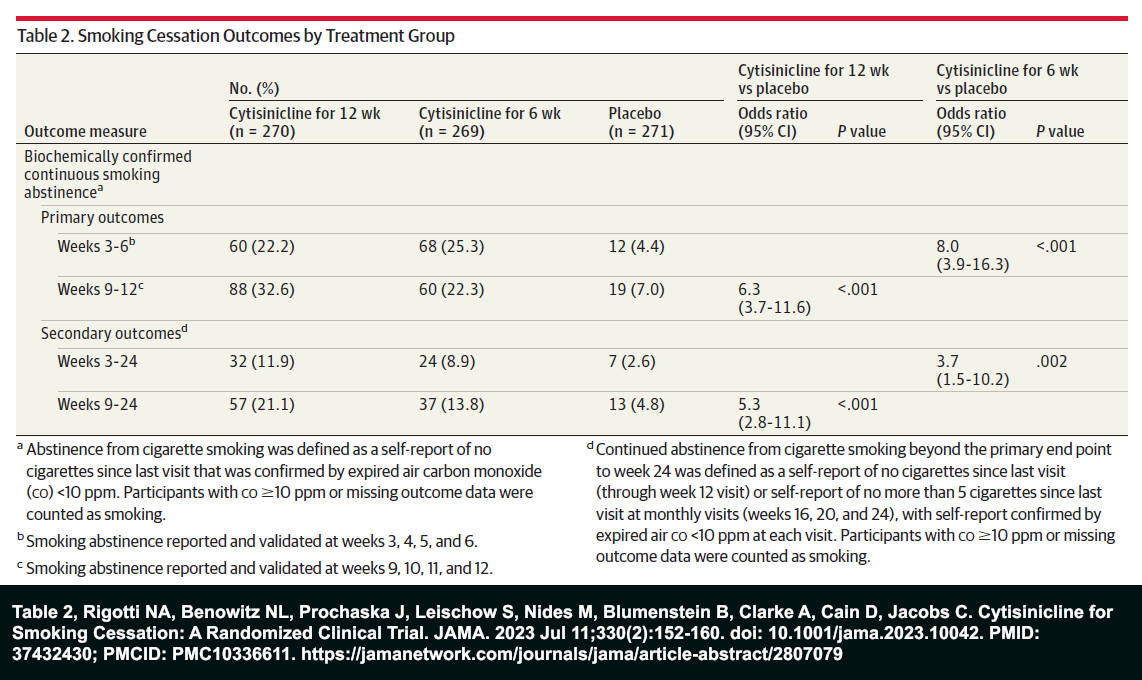
Published by The Journal of the American Medical Association (JAMA) on July 11, 2023, and entitled "Cytisinicline for Smoking Cessation: A Randomized Clinical Trial" (ORCA-2), the Achieve Life Sciences sponsored study involved 810 U.S. smokers recruited by 16 corporate research centers and 1 hospital in 17 mostly eastern states.
Smokers were randomized to one of three study arms: (1) 270 quitters assigned to 12 weeks of 3 mg. cytisinicline tablets taken 3 times daily, (2) 269 quitters assigned to 3 mg. cytisinicline tablets 3 times daily for 6 weeks, followed by 6 weeks of placebo tablets 3 times daily, or (3) 271 quitters assigned to placebo tablets 3 times daily for 12 weeks.
Participants also attended 15 behavioral support sessions through study week 12. Sessions were conducted by trained counselors and lasted up to 10 minutes each. Three additional shorter sessions occurred during follow-ups at weeks 16, 20, and 24. All participants were instructed to stop smoking 5 to 7 days after beginning the use of study tablets.
ORCA-2 Findings
As shared in ORCA-2 Table 2, the highest continuous smoking abstinence rate over the longest period monitored (weeks 3 to 24) was 11.9% and occurred in the 12-week cytisinicline treatment arm, compared to 8.9% in the 6-week arm, and 2.6% for placebo.
While cross-study comparisons are frowned upon as populations and study conditions differ, the ORCA-2 24-week 11.9% outcome is strikingly similar to the 11.7% 6-month 1.5mg cytisine continuous abstinence rate generated in Courtney 2021.
Courtney was a large minimal contact randomized trial involving 1,452 participants. It pitted a standard/historic 25-day downward titrated course of 1.5 mg. cytisine against a standard 84-day course of varenicline. Generating a 13.3% 6-month rate, varenicline didn’t fare much better.
How meaningful is ORCA-2's week 3-24 continuous abstinence rate when 88.1% of frequently counseled and supported 12-week cytisinicline users were smoking within 24 weeks? Even there, the definition of “continuous abstinence” was fudged a bit.
Participants who smoked up to 5 cigarettes in the month before study visits at weeks 16, 20, and 24 were considered continuously abstinent so long as they claimed to have quit again and their breath test for expired carbon monoxide was less than 10 parts per million. Normally, smoking is undetectable by breath tests within 24 hours of not smoking.
Support’s Efficacy
The study’s authors concluded that “cytisinicline, along with behavioral support, has robust efficacy and excellent tolerability as a treatment for tobacco dependence.”
“Along with behavioral support”?
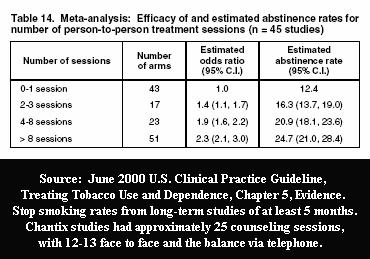
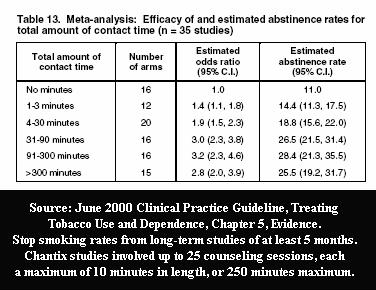
The number of ORCA-2 behavioral support sessions (18) and study contact time (up to 150 minutes, plus 3 additional “shorter” sessions) generated independent efficacy.
Given that nearly all real-world quitting product use occurs without the benefit of ongoing professional counseling, how much of the study’s outcome is attributable to cytisinicline, and how much to support?
Partial Agonists
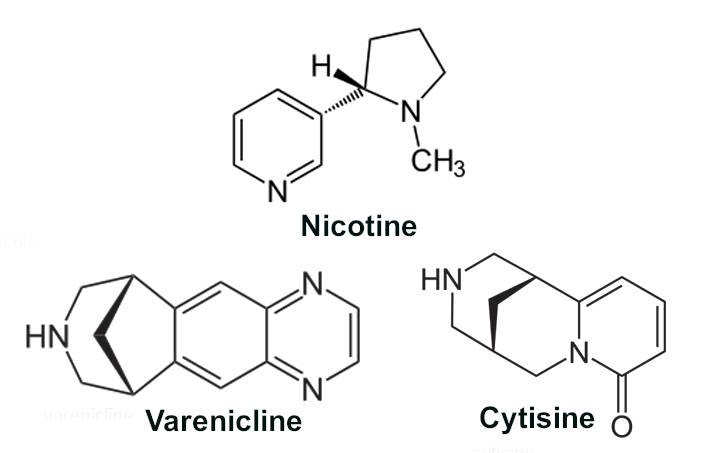
Sharing molecular architecture with both nicotine (C10H14N2) and varenicline (C13H13N3), researchers understandably contrast cytisine (C11H14N2O) with varenicline. Varenicline was sold exclusively by Pfizer as Chantix or Champix before its 2020 patent expiration, Chantix’s 2021 recall, and the FDA’s 2021 generics authorization.
Both are dopamine pathway receptor (nAChR) partial agonists, with receptors having 7 times higher affinity for cytisine than nicotine, yet 5 times lower affinity than for varenicline.
When receptor binding strength is coupled with drug elimination half-lives of roughly 2 hours for nicotine, 5 hours for cytisine, and 24 hours for varenicline, and the fact that, so far, there appears to be “significantly fewer adverse events with cytisinicline than with varenicline,” it’s easy to understand researcher excitement about cytisine’s ability to block 30% of nicotine receptor binding while providing 56% of nicotine’s agonistic wanting satisfaction and satiety effects.
But, again, how meaningful is cytisine’s ORCA-2 efficacy when two comparable 2006 varenicline (Chantix) FDA approval studies (Gonzales and Jorenby) generated significantly higher 24-week continuous smoking cessation rates than cytisinicline (29.5% and 29.7% vs. 11.9%), yet lower efficacy (3.68 and 2.83 vs. 5.3)?
Continuing to conflate efficacy with effectiveness, the National Cancer Institute (NCI) and Centers for Disease Control (CDC) have openly anointed varenicline as the most effective stand-alone quitting product.
Of note, varenicline FDA approval studies involved more participant contact than ORCA-2. The Gonzales and Jorenby studies involved up to 160 minutes of counseling time (16 sessions up to 10 minutes each), plus 8 additional support telephone calls of unknown duration.
Why care? Leas 2017 was a national population-level effectiveness survey published in the Journal of the National Cancer Institute. Possibly the most detailed propensity score matching study ever, it found that compared to non-users, there was “no evidence that use of varenicline, bupropion or nicotine replacement increased the probability of 30 days or more smoking abstinence at one-year follow-up.”
According to Leas, “The lack of effectiveness of pharmaceutical aids in increasing long-term cessation in population samples is not an artifact caused by confounded analyses. A possible explanation is that counseling and support interventions provided in efficacy trials are rarely delivered in the general population.”
The real-world ineffectiveness of FDA-approved quitting products isn’t news.
Between 1984 and June 2000 more than a hundred placebo-controlled randomized clinical trials found the 6-month clinical efficacy of nicotine replacement therapy (NRT) roughly double that of placebo.
Then, after analyzing 3 waves of real-world survey data (1992, 1996, and 1999) from 5,247 participants, a 2002 JAMA study concluded that "Since becoming available over the counter, NRT appears no longer effective in increasing long-term successful cessation in California smokers."
Since then, in nearly all hands-off population-level observational studies, smoking cessation’s real-world emperor, OTC NRT, has consistently remained naked yet rich.
Achieve’s ORCA Studies
Achieve Life Sciences is the driving force behind all ORCA studies. ORCA is the company’s pseudo mark for “Ongoing Research of Cytisinicline for Addiction.” Pending FDA approval, Achieve’s goal is the manufacture and sale of cytisinicline for both smoking cessation (ORCA-1, ORCA-2, and ORCA-3) and vaping cessation (ORCA-V1).
Was the ORCA-2 study financially independent? No. The JAMA study’s “Conflicts of Interest Disclosure” notes that all nine study authors are either employed by or received grants or personal fees from Achieve Life Sciences.
Achieve’s March 16, 2023 Form 10-K SEC filing makes clear that cytisinicline is the corporation’s sole product and that Achieve is betting its survival on FDA approval, followed by robust sales.
Future Marketing Representations
Choosing 5 additional letters in distancing “cytisinicline” from existing “cytisine” products, the elementary marketing integrity question is, should real-world cytisinicline users expect to experience 5 times greater odds of success? No, and I’m confident Achieve knows it. And it matters.
How many of the 11 million U.S. adult e-cigarette users were super frustrated smokers who surrendered to vaping after decades of crashing and burning while using products that the FDA promised would double their quitting chances?
While the Federal Trade Commission continues to allow the NCI, FDA, and manufacturers to shout that nicotine replacement products (NRT) “doubles your chances,” nearly all population-level observational study findings have found over-the-counter NRT ineffective when compared to non-users, unassisted quitters, or cold turkey.
While Achieve’s cytisinicline appears poised to gain FDA approval, what success representations will it be allowed to make in motivating smokers to hand over their money?
Before approval, will the FDA demand evidence of the value of 84 days of 3mg. of cytisine taken three times daily, when unaccompanied by ongoing professional counseling or support?
Will smokers be informed that Achieve’s ORCA-2 study found that just 1 in 8 12-week cytisinicline users who received up to 18 counseling sessions achieved sustained smoking abstinence from weeks 3 to 24?
And will they be told that, although half the dose of cytisinicline, natural and substantially less expensive cytisine products are available?
Nicotine Dependency Recovery
While ORCA-2 states that cytisinicline offers “new nicotine dependence treatment options,” the study appears to have ignored testing body fluids (saliva, blood, or urine) to determine if participants successfully stopped using nicotine and arrested their dependence.
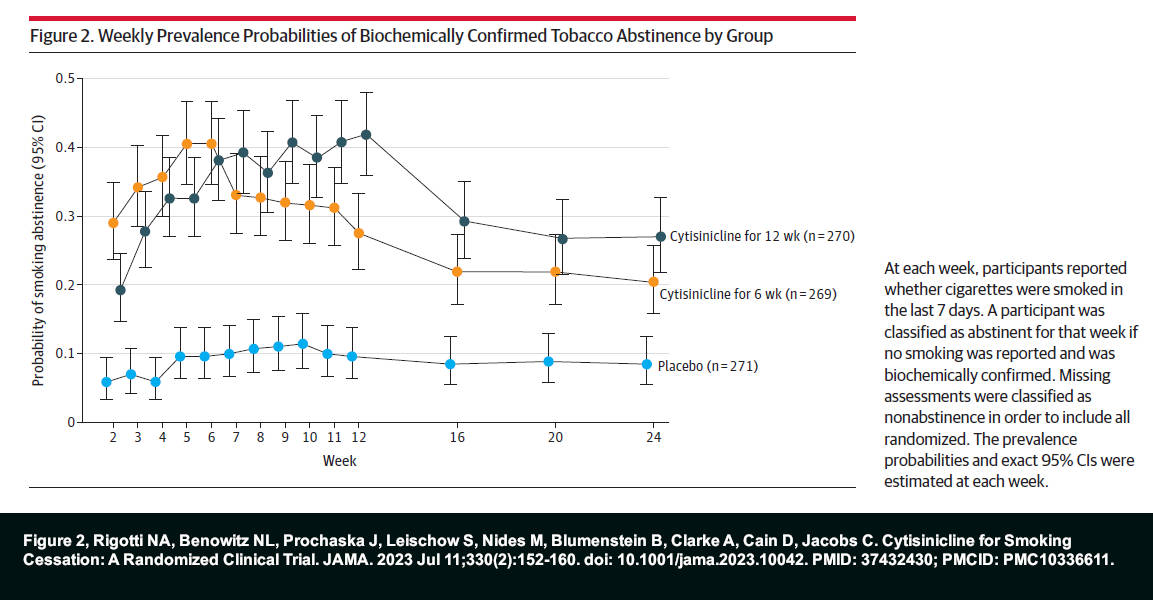
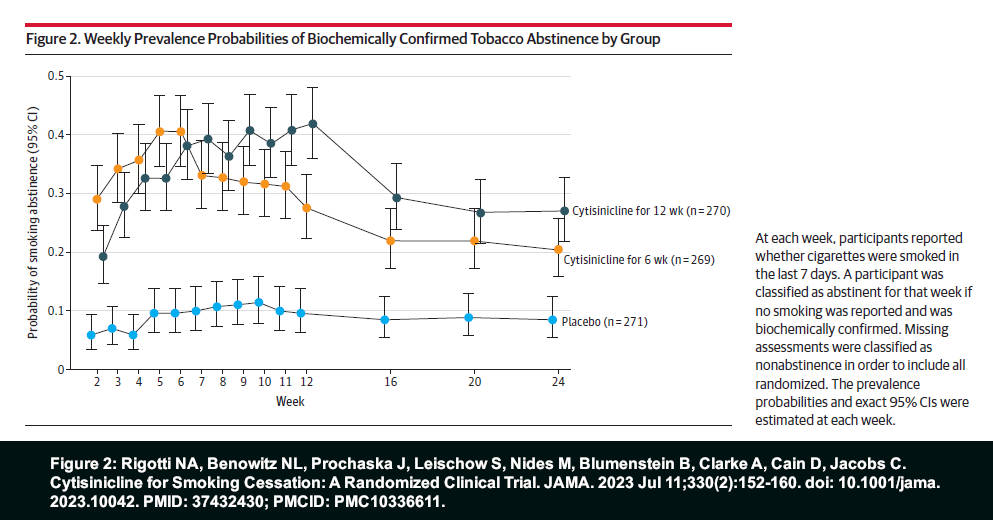
While smoking abstinence rates normally gradually decline during and after treatment, the 12-week ORCA-2 cytisinicline treatment arm experienced 5 weekly cessation increases beyond treatment week 4 (see Figure 2).
What percentage of cytisinicline users switched to replacement nicotine, smokeless tobacco, or vaped nicotine, and remained nicotine dependent? We don’t know. But neither does Achieve or the FDA.
If Achieve wants to continue making “nicotine dependence treatment” representations, it needs supporting evidence.
The per-participant cost for end-of-treatment or end-of-study urine testing with 99% accuracy in detecting cotinine, nicotine’s primary metabolite, is roughly $1.00.
Achieve’s “Natural” Competitors
Cytisine, also known as baptitoxine, sophorine, or cytisinicline, is found in the Faboideae plant family. As with nicotine, an animal toxic alkaloid, it’s extracted from the seeds of cytisus laburnum trees and shrubs. Also known as golden chain, the trees grow up to 23 feet tall and are native to calcium-rich soils of central and southern Europe.
First sold in Bulgaria in 1964 as a 25-day over-the-counter (OTC) stop smoking aid/program called Tabex, the cost of a box of 100 1.5mg tablets is $25.00. The same dose and number of pills are marketed by a Polish company as Desmoxin and are available on Amazon for $23.74.
As if attempting to distance and distinguish itself from OTC natural cytisine, ORCA-2 repeatedly refers to cytisinicline as “medication.”
ORCA-2 Blinding Integrity
Is the FDA troubled by ORCA-2’s 2.6% 24-week placebo rate?
Contrasting varenicline approval study findings, it’s 4 times lower than the 10.5% 24-week placebo continuous abstinence rate in Gonzales, and 5 times lower than the 13.2% rate in Jorenby.
Gonzales and Jorenby are closer to the average 6-month placebo rate of 12.06% generated by 72 placebo study arms presented as evidence supporting the June 2000 US Tobacco Cessation Guideline.
Averaging 52.5 years of age, ORCA-2 participants were older and more experienced than smokers normally seen in quitting studies. For example, the average quitter was 42.6 in Jorenby and 42.3 in Gonzales.
Heavy smokers and experienced quitters, ORCA-2 participants averaged 19.4 cigarettes per day and averaged 4 prior quit smoking attempts.
Roughly a third of those attempts involved experiencing the dopamine satiety effects of using FDA-approved products: varenicline (354), replacement nicotine (512), and bupropion (153).
ORCA-2 study recruiting advertising -- used to entice smokers to participate -- expressly fostered a hope or expectation of receiving “3.0 mg cytisinicline in combination with behavioral support.” Cytisinicline expectations may be greater in Achieve’s ORCA-3 trial, as reviewed ads make no mention of the possibility of receiving placebo tablets instead (03/27/22 and 10/01/22).
Like all placebo quitters, ORCA-2’s inert tablet takers experienced peak nicotine withdrawal within 24 to 48 hours of stopping smoking. What percentage had become highly skilled at recognizing the onset of their withdrawal syndrome?
While ORCA-2 participants were allowed to take their assigned tablets for a full week before being required to stop smoking, according to Figure 2, roughly 94% of the placebo arm had relapsed to smoking by week 2.
By then, smoking and frustrated, what value were the study’s 14 remaining behavioral support sessions to them?
Cessation blinding concerns aren’t news to researchers. They are keenly aware that nicotine is a psychoactive chemical, a central nervous system stimulant that also stimulates the release of dopamine.
They also know that nicotine cessation produces withdrawal symptoms often characterized by anxiety, anger, dysphoria, concentration difficulty, and sleep fragmentation within 24 hours of quitting.
How bad is assignment awareness? The primary study used to gain FDA approval of Nicorette nicotine gum, Jarvis 1982, resorted to the extreme of using “a placebo containing 1 mg of nicotine, but unbuffered.”
Although study placebos were normally provided by the manufacturer of the product being evaluated, researchers in several nicotine patch studies also acknowledged using active placebos containing small amounts of nicotine (Campbell 1996, Sonderskov 1997, and Ahluwalia 2002).
Entitled “The blind spot in the nicotine replacement therapy literature: assessment of the double-blind in clinical trials,” Mooney 2004 found that placebo-controlled NRT trials were generally not blind as claimed, as participants could correctly declare their assignment at rates significantly above chance.
The study warned researchers that "the validity of NRT clinical trial results could be questioned" if future studies failed to make proper blinding integrity assessments. It’s a warning that nearly all subsequent studies ignored.
Were ORCA-2 efficacy victories the result of frustrated and/or fulfilled expectations, or cytisinicline’s actual relative worth?
The FDA was provided detailed notice of the history of smoking cessation study blinding concerns in February 2019. Given ORCA-2’s dismal 2.6% placebo rate, is the FDA demanding blinding integrity assessments? If blinding concerns are found, will the study's findings be adjusted accordingly?
Given that nearly the entire ORCA-2 placebo arm relapsed by week 2, the optimum time to ask participants to declare or guess their randomized assignment is within 2 weeks of quitting, while memories are fresh.
The ultimate unaddressed questions are, if we’ve known for two decades that placebo-controlled smoking cessation trials are not blind, why pretend that they are, why allow placebo comparisons to dominate the cessation science base, and why continue to conduct them, especially in light of ethical concerns?
ORCA-2’s Unique Population
In stark contrast to smokers seeking free quitting products and willing to delay quitting until commanded to do so by researchers, roughly half of real-world attempts are spontaneous. Spur of the moment decisions, the smoker simply decided it was time.
Impossible to evaluate in randomized trials such as ORCA-2, two real-world studies found that spontaneous unplanned stop smoking attempts were 260% more likely to succeed than planned ones (West 2006 and Ferguson 2009).
Also absent from cytisinicline studies are all quitters who “plan” to quit cold turkey (most quitters), smokers quitting unassisted, or those who plan to use counseling or support resources, unaccompanied by quitting product use.
While ORCA-2 randomized 810 volunteers, it intentionally excluded 504 for being ineligible.
Among those excluded were current marijuana users, smokers who also vaped, those with uncontrolled hypertension, kidney impairment; a history of acute myocardial infarction, unstable angina, cerebrovascular incidents, hospitalization for congestive heart failure, those with moderate depression or worse, smokers with a diagnosis of schizophrenia, bipolar disorder, current psychosis, at risk for suicide, or who had a positive urinary screen for illicit drugs.
Might cytisinicline benefit some quitters more than others? It’s possible. But with Achieve swinging for the fence, it could be decades before infield hits get noticed.
Cytisinicline isn’t alone. Unlike real-world observational studies, randomized quitting product trials are inherently exclusionary of the vast majority of quitters. It’s why “your chances” claims flowing from them are inherently unfair and highly deceptive.
Cytisine/Cytisinicline Safety
While comforting that Tabex cytisine tablets have been sold in Eastern Europe for nearly 60 years without generating use-risk headlines, Achieve has doubled tablet strength from 1.5mg to 3mg. while tripling the treatment period from 25 to 84 days.
While a Tabex user consumes 150mg. of cytisine over a 25-day treatment course, ORCA-2 cytisinicline quitters consumed 225mg. within 25 days, a 50% increase.
According to ORCA-2 Table 3, the study documented 494 adverse events in the 12-week treatment arm, 459 in the 6-week arm, and 359 among placebo quitters.
It notes 8 “serious adverse events” occurring in the 12-week cytisine arm (3% of the arm), 10 in the 6-week cytisine arm (4%), and 3 in the placebo arm (1%).
A serious event was defined as “an adverse event that resulted in death or was life-threatening; required hospitalization or prolonged an existing hospitalization; resulted in persistent or significant disability, incapacity, or congenital abnormality; or which required medical intervention to prevent any of the above outcomes.”
During ORCA-2, 10 participants in the 12-week cytisine arm withdrew from the study compared to 6 in the 6-week cytisine arm, and 4 taking placebo tablets.
While the study’s authors assure us that, “No serious adverse event was judged to be treatment-related, including the 1 death that occurred in the 6-week cytisinicline group,” the FDA is hopefully giving safety significant scrutiny.
The most common and notable cytisine adverse events reported by ORCA-2 were insomnia (which occurred in 9.5% of the study’s 539 cytisine users vs. 5% among its 270 placebo quitters), abnormal dreams (cytisine 8% vs. placebo 3%), constipation (cytisine 5.5% vs. placebo 1%), and anxiety (cytisine 4.5% vs. placebo 2%).
Dale 1912 opens by noting that in 1888 Radziwillowicz documented 131 cases of accidental cytisine poisoning, including 3 deaths. They mostly occurred in children after eating seeds from the laburnum tree, but also after cooking while mistakenly using laburnum flowers as an ingredient.
The most consistent symptom was vomiting, which could be followed by delirium, hallucinations, pupil dilation, muscular twitching, cold sweats, and convulsions, with death due to respiratory paralysis.
Although pregnant women are not mentioned as having been excluded from ORCA-2, what are the consequences of the toxin cytisine upon the developing fetus?
Świątkowski 2023 evaluates nicotine and cytisine embryotoxicity in zebrafish. Published in August, the study found that, unlike nicotine, while cytisine did not produce death for the various concentrations tested, it did delay hatching in 67-100% of animals. Cytisine decreased heart rate at the highest concentration while reducing the development of pigment at a lower concentration.
Ongoing cytisine safety research is needed, especially for all ORCA-2 excluded conditions.
Closing Thoughts
Although I’d love to be wrong, future real-world observational cytisinicline findings won’t be kind.
But by then, FDA drug approval credibility and USDHHS marketing will be so heavily invested that, at all costs, the truth must and will be sacrificed.
Try to locate any reference to any smoking cessation observational effectiveness finding on any FDA, NCI, or CDC webpage. Good luck.
In 2003, Simon Chapman was a professor of public health at the University of Sidney and editor of the journal Tobacco Control. That year he resigned from a GlaxoSmithKline (GSK) funded consortium in protest over GSK attempting to block new Zyban (bupropion) controls after dismal real-world performance.
Twenty years later, the title of Professor Chapman’s newest book says it all, “Quit smoking weapons of mass distraction.”
What’s needed? Long overdue yet meaningful in-depth research into how most quitters succeed.
If the vast majority who successfully arrest their dependence upon nicotine are doing so by quitting cold turkey, what are the keys to successful abrupt nicotine cessation and why are the FDA, NCI, and CDC not openly and eagerly sharing them, while celebrating free quitting's value?
A billion dependency-related deaths expected during the 21st century, it's not too late.
 John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," 6 peer-reviewed journal articles, and founder and director of Turkeyville, a 17,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com
John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," 6 peer-reviewed journal articles, and founder and director of Turkeyville, a 17,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}