
Is Truth Initiative truthful about how smokers quit?

Image by Gerd Altmann (geralt)
With $833 million in assets, the Truth Initiative Foundation (“Truth”), formerly the American Legacy Foundation (1999-2015), is America’s wealthiest non-profit dedicated to battling nicotine addiction. According to the foundation’s bio, “We investigate, expose, and amplify the truth about smoking, vaping, and nicotine.”
A talented staff of roughly 140, they hopefully feel pride in having been the lead youth smoking prevention organization responsible for driving U.S. youth smoking rates to record lows.
But when it comes to smoking cessation and nicotine dependency recovery, respectfully, in multiple regards, Truth's record is disappointing.
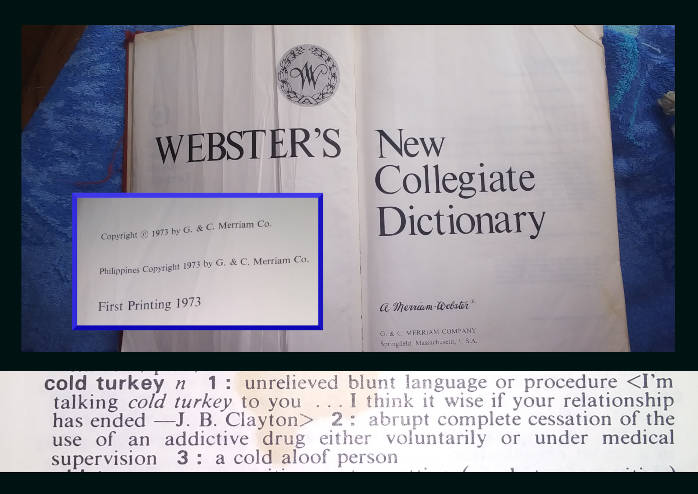
“Cold Turkey” Defined
“Cold turkey” has historically been defined as "abrupt complete cessation of the use of an addictive drug either voluntary or under medical supervision."
The problem? Truth Initiative is openly hostile to quitting cold turkey, suggesting that it’s nearly impossible with few able to successfully quit.
Cold Turkey "Doesn't Work"
According to Google, Truth’s leading page discussing “cold turkey” is titled "Why the 'cold turkey' method of quitting vaping or smoking doesn’t work – and what does."
Published on December 1, 2022, readers are told that “Whether it’s cigarettes, e-cigarettes, or any other tobacco product, trying to quit 'cold turkey' – meaning to stop abruptly without any support or replacement medications – is unlikely to be successful.”
Attributed to Dr. J. Taylor Hays, who serves as director of the Mayo Clinic Nicotine Dependence Center, Truth tells smokers contemplating cold turkey that “research over the past 25 years has shown that out of 100 people trying to quit smoking cold turkey, only about three to five of them will succeed for longer than six months. In other words, while some people can quit this way, at least 95% of people can’t.”
First, reflect on the absurdity of redefining cold turkey to exclude all cold turkey quitters supported by family, friends, their doctor, nicotine addiction experts, a cold turkey quit smoking booklet, an app, a website, or a support group.
It’s my experience that those attempting to shrink the giant bird in the room are usually either selling quitting products or programs, accepting donations from those who are, or who have vested substantial credibility in their use.
The 1998 Tobacco Master Settlement Agreement (MSA) created the national foundation that is today known as the Truth Initiative (see PDF page 25). Encompassing both prevention and cessation, MSA Section VI(a) makes the foundation’s primary purpose “the study of and programs to reduce youth tobacco product usage and youth substance abuse in the States.”
What’s unsettling is Truth suggesting to nicotine-dependent teens visiting its website that “replacement medications” are more successful than cold turkey when: (1) the FDA has not approved the use of “replacement medications” by teens; and (2) when 2006, 2013, and 2017 meta-analytic studies in the Cochrane database have found adolescent use of replacement nicotine ineffective.
Also disturbing is Truth’s suggested take-away, that 95% of smokers “can’t” quit cold turkey. Really?
Back in 2002, even GlaxoSmithKline (GSK), which makes and sells nicotine gum, patches, and lozenges, was doubling Truth’s measly 5 percent. According to GSK's Australian website, “In one study over 90% of cold turkey quitters were smoking again after six months.”
Truth's "three to five" percent reference is likely from Hughes 2004 which concluded that "3–5% of self-quitters achieve prolonged abstinence for 6–12 months after a given quit attempt." What readers are not told is that those rates have little relationship to cold turkey quitting.
They reflect control or placebo group rates from 15 smoking cessation clinical trials involving quitters who sought treatment. It's a point the study's authors openly acknowledge in alerting researchers to the fact that "we need survival curves describing the outcome of unaided quitting. Surprisingly, we did not find a single true survival curve among true self-quitters; i.e. those who do not seek treatment."
The Hughes 2004 authors didn't hide their motivation for the study. The shared rationale was that the 2000 Clinical Practice Guideline for Treating Tobacco Use and Dependence (2000 Guideline) had identified some interventions having only 5-9% 6-month efficacy.
"These low rates prompt many to question whether these interventions are effective," wrote the authors. "A replication that rates of [long-term prolonged abstinence] in studies of untreated smokers are less than 5% could reassure critics that such interventions might be effective."
It should be noted that a common statement seen in Truth smoking cessation studies is that Truth's programs are developed "in accordance with the Clinical Practice Guidelines for Treating Tobacco Dependence."
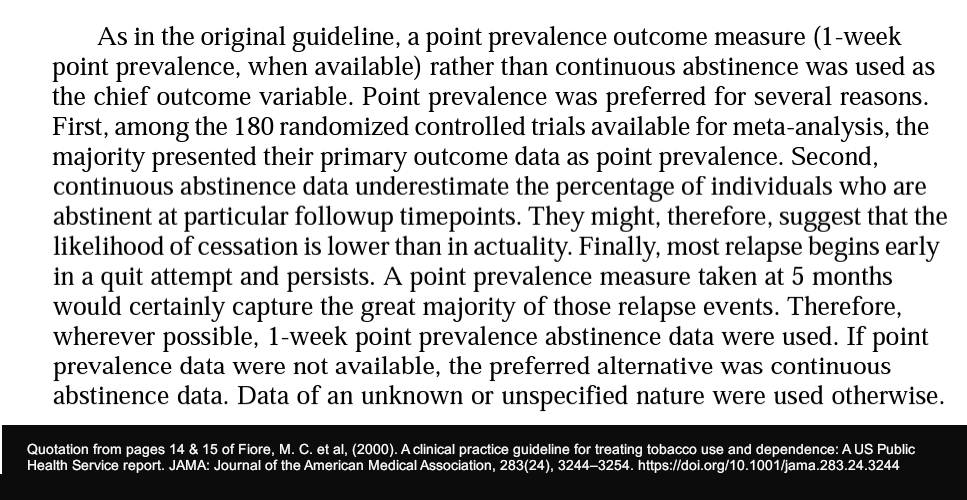
What Truth doesn't mention when sharing the "3-5%" finding is that Hughes 2004 presents more stringent continuous abstinence rates, while the chief outcome measure used by both the 2000 Guideline and the 2008 Update is point-prevalence abstinence.
With continuous abstinence, quitters needing a couple of days or attempts to get started are counted as failures 6 months later.
Point-prevalence, not continuous abstinence, is also the standard used in most Truth cessation studies.
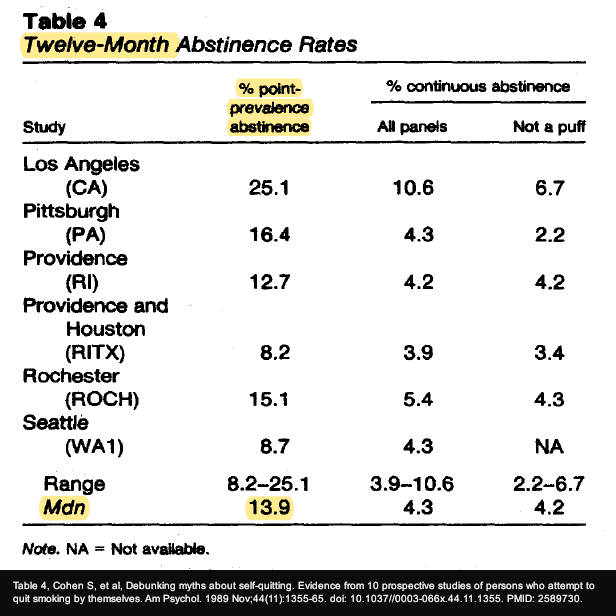
How big a difference can it make? Hughes 2004 states that 10 of the 15 studies used to generate its "3–5%" finding were reviewed by the Cohen 1989 study. There, according to Cohen Table 4, 13.9% of all self-quitters analyzed by the study achieved 12-month point-prevalent abstinence.
"Read This Before" Going Cold
A second page entitled “Read this before trying to quit smoking 'cold turkey'” is the top Truth page returned by smokers and quitters searching Google for "tips on quitting smoking cold turkey."
Dated December 17, 2017, it mirrors the claims made on Truth’s cold turkey “doesn’t work” page before referring readers to a 10 steps" planning page, where step 5 is "Choose a quit smoking aid" ... "such as gum, the patch, inhaler or prescription meds like Chantix or Zyban."
Some more than others, additional TruthInitiave.org pages bashing cold turkey include “3 tips for boosting success with an online quit-smoking program” (April 12, 2018), a PDF entitled “Quitting Smoking” (Nov. 2018), “How to quit JUUL” (Feb. 7, 2019), “Quitting smoking is more important than ever – here is how to get started now” (April 20, 2020), “How to support someone on their quit-vaping journey” (March 2, 2023) and “3 important things to know about quitting nicotine during times of stress” (March 23, 2023).
Question. Over the years, how many cold turkey quitters crashed and burned following flame-outs caused by Truth pouring ice water on their attempt? Most were likely searching for help and were clubbed with discouragement instead.
What teen who is almost through the up to 72 hours needed to empty their brain and bloodstream of nicotine and move beyond peak withdrawal would continue after repeatedly being hammered with the message that almost all cold turkey attempts fail?

Cold Turkey Works!
Now, contrast Truth’s proclamation that cold turkey “doesn’t work” with the following paragraph from page 15 of the 700-page 2020 treatise entitled “Smoking Cessation: A Report of the Surgeon General” (full PDF):
“Proponents of encouraging smokers to quit without treatment, often called quitting "cold turkey," point to data indicating that most smokers who quit successfully do so without medications or any type of formal assistance, as well as to population surveys suggesting that cold-turkey quitters do as well or better than those who use over-the-counter NRTs. Proponents of this approach also suggest that medicalization may disempower smokers and create artificial barriers to quitting (Alpert et al. 2013; Polito 2013).”
While the Surgeon General’s report goes on to explore theories as to why observational findings differ from clinical trials, the findings themselves are not in question.
And compare the Surgeon General noting that most successful ex-smokers quit cold turkey with Truth’s November 2018 “Quitting Smoking” fact check PDF claiming that, “Most smokers who attempt to quit do so ‘cold turkey’ and are not successful.“
Page 2 of Truth's fact check blames cold turkey for contributing to the nation's low quitting rate. "Nevertheless, annual quit success rates remain low — at roughly 7 percent — underscoring the highly addictive nature of nicotine, the ineffectiveness of the “cold turkey” approach, or not using available treatments, and the multiple attempts it can take to successfully quit3," Truth writes.
The source supporting footnote 3 - a 2017 CDC MMWR - doesn't mention cold turkey or present any evidence that it's ineffective.
Also, contrast the Surgeon General’s acknowledgment that “most smokers who quit successfully do so without medications or any type of formal assistance,” with Truth’s August 2020 assertion that “Quitting smoking is not something people should do on their own.”
So, what’s the truth? Who should adolescent, young adult, and adult smokers believe?
Weapons of Mass Distraction
Published in 2022 and authored by Professor Simon Chapman, a former editor of the journal Tobacco Control, “Quit smoking weapons of mass distraction” (free PDF) presents evidence that the vast majority who successfully arrest their chemical dependence have done so unassisted or cold turkey.
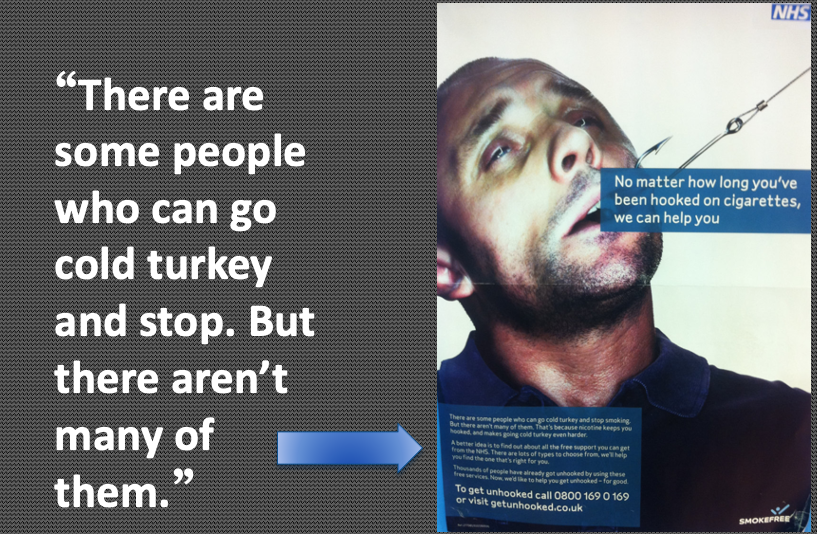
In Weapons, Chapman is shocked by the caption beneath a 2008 UK NHS poster showing a man resisting a taught line tugging on a fishing hook penetrating his cheek. The caption reads, "There are some people who can go cold turkey and stop. But there aren't many of them."
Sound familiar?
"When I first saw it I was gobsmacked by the outrageously incorrect statement," writes Chapman. "'But there aren't many of them' (who quit cold turkey) is completely and utterly wrong. It's a weapons-grade lie, which as we have seen is easily contradicted by data going back several decades to at least the 1960s."
Efficacy vs. Effectiveness
Truth knows that smokers wanting to quit cold turkey generally don’t join randomized clinical trials dangling free quitting products as study recruiting bait.
It also knows that clinical efficacy findings have conflicted with observational effectiveness since at least 2002, when a Journal of the American Medical Association study concluded that "Since becoming available over the counter, NRT appears no longer effective in increasing long-term successful cessation in California smokers."
MSA Section IV(f)(4) charges Truth with “developing and disseminating criteria for effective cessation programs; monitoring and testing the effectiveness of such criteria; and continuing to develop and disseminate revised versions of such criteria, as appropriate” [emphasis added].
While most quit attempts are cold turkey, and 40-50% are spontaneous with little or no planning (both West 2006 and Ferguson 2009 found unplanned attempts 240% more likely to succeed), clinical trials are generally populated by smokers seeking free treatment, a non-existent real-world population willing to delay quitting until commanded by researchers to begin.
The quitting product industry, their consultants, and 5-day residential quitting programs charging $4,800 (exclusive of hotel and quitting product costs) have obvious financial motives for needing to portray free cold turkey quitting as nearly impossible.
Did Truth's initial 1999 cessation naivety collide with its Section IV(f)(4) mandate to discover what works, motivating it to embrace and megaphone the quitting industry's sales pitch?
What possible motive could Truth have for representing clinical efficacy as population-level effectiveness, for equating the low success rates of people who are randomly assigned to receive a placebo or no treatment in clinical trials as being cold turkey quitters?
Extreme selection bias in excluding all spontaneous, cold turkey, and unaided quitters, randomized trials not being truly blind in nicotine being psychoactive and withdrawal being nearly impossible to miss, the timing and content of counseling and support often tailored to aid successful transfer to the agonist or partial agonist being evaluated, should we be surprised that efficacy and effectiveness findings are almost diametric opposites?
And reflect on the dependency satiety bias associated with measuring and comparing the accomplishment of quitters abruptly ending chemical stimulation of α4β2-type nicotinic receptors, to those who delay ending stimulation for weeks, months, or indefinitely.
Imagine comparing alcoholics who quit drinking to those on an alcohol IV drip. How long before someone shouts fraud?
Science? Smoking's deadliness compromised common sense on June 22, 1983, the day that the first NRT product, Nicorette nicotine gum, was recommended for approval.
Little difference between then and now, the cigarette's deadliness and relative risks continue to discourage most from shouting the truth, that vaping is harmful and diminishes quality of life.
Why, since 2004, has Philip Morris taught smokers that NRT is a key to successful quitting? Why have we never once heard a Nicorette or Chantix commercial tell smokers why they need to quit, because smoking kills?
At war with the neo-nicotine industry's desire to addict the planet, failure to reflect on the historic partnership between the tobacco and pharmaceutical industries dooms future generations to either figure out addiction on their own or remain nicotine's slave until the day they die.
Distracted, what's needed is for Truth to become worthy of its name.
A big-picture starting point in adherence to the MSA Section IV(f)(4) requirement to monitor effectiveness would be to obtain a complete and accurate picture of the productivity and effectiveness of all nicotine cessation and switching methods.
Hands-off observational studies could also include analysis of support available to all methods, including quitting programs, support groups, counseling, books, websites, apps, and text messaging.
There's little debate but that the highest quality observational studies are prospective, following the same users over time, while employing propensity score matching.
Propensity score matching allows us to draw conclusions about cause and effect. They do so by greatly diminishing the risk of confounding, by grouping participants who are similar in all respects except for the quitting method. It allows us to more reliably compare core quitting or dependency transfer methods, including the value of method accompaniments.
Despite MSA Section IV(f)(4) twice expressly requiring it, except for the foundation’s early days (1999-2003), Truth has generally ignored quitting method evidence of population-level effectiveness and productivity.
Pregnancy Quitters
For example, a May 2023 study found that among 2,477 pregnant smokers who attempted to quit, 74.4% chose cold turkey (unassisted).
Unaided mothers-to-be generated an adjusted effectiveness rate substantially higher than for women attempting to transfer to vaping (44.6% vs. 31.2), and 2.4 times higher than a combined group that pooled all remaining methods, including NRT quitters (the nicotine patch, gum, lozenge, spray or inhaler), bupropion and varenicline (44.6% vs. 18.9%).
As noted by the authors, “Our findings highlight the opportunity for presenting the positive message about unassisted cessation as the most common and successful quitting method to pregnant smokers who are ready to try to quit.”
What quitting method advice is Truth sharing with pregnant smokers?
Truth has a page entitled “Answers to 8 common questions about smoking and pregnancy.” After telling women that getting support is important, it encourages them to join BecomeAnEx, a free cessation support site that discourages cold turkey quitting. The site was developed and is managed by Truth in partnership with the Mayo Clinic Nicotine Dependence Center.
There, the Mayo Clinic's Dr. Richard D. Hurt advises them that there are quitting medications safe to use during pregnancy and to talk to their doctor if in need of help.
Invited in 2006 by leading nicotine toxicologists to bring a cessation perspective to “Critical Review: Nicotine for the Fetus, the Infant and the Adolescent?”, I was horrified to learn that nicotine can damage the first-trimester embryo by altering the trajectory of normal brain development.
According to research by Professor Theodore A. Slotkin, a Duke Medical University toxicologist, nicotine disrupts normal brain development by activating acetylcholine receptors prematurely and with inappropriate intensity, before the brain neuron the receptor is attached to has had an opportunity to fully develop and properly interface with surrounding brain neurons.
I recall University of Arkansas physician and toxicologist K.H. Ginzel worrying about England experiencing a substantial IQ shift to the left after several UK “experts” recommended replacement nicotine use by pregnant women and 12-year-olds in 2005.
Adolescent Quitters
Despite MSA Section IV focusing almost entirely on youth tobacco product use and Section IV(f)(4) specifically charging Truth with "developing and disseminating criteria for effective cessation programs," 25 years later, what free cessation program does Truth sponsor or recommend in helping America's roughly 320,000 middle and high school smokers quit?
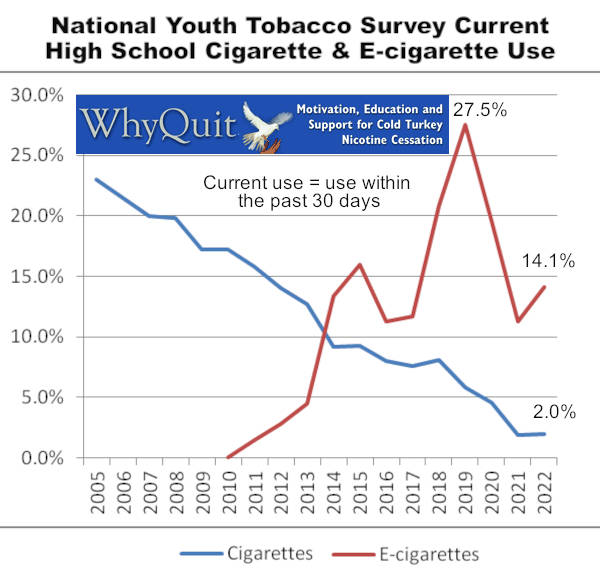
According to the 2022 National Youth Tobacco Survey (NYTS), roughly 17 million U.S. high school students (public + private grades 9-12) used e-cigarettes in 2022, with 2.1 million (14%) vaping within the past 30 days, and 640,000 (3.7%) vaping every day.
Most disturbing are the 40,000 U.S. middle school students already slaves to daily vaping. Time bombs headed towards high school, most are skilled at smoke tricks while craving peer acceptance.
Who do we have to thank for our national youth survey? Truth’s initial Section IV(f)(4) investigative instincts were spot-on.
In 1999, Truth (then the Legacy Foundation) partnered with the CDC in sponsoring the first National Youth Tobacco Survey. While the 1999 survey didn’t ask about adolescent quitting, the 2000 survey report did.
There, Truth learned that among 319 daily smokers aged 11-19 who had successfully quit smoking, 93.6% had not used any of the 5 quitting choices the survey had asked them about (the nicotine patch or gum, Zyban, a telephone quit-line, a school cessation program, or a community program).
Which method wasn't mentioned?
In this era of ever-increasing nicotine transfer and weaning schemes, it’s critical to include a short definition of cold turkey when asking about methods. Suggestion: cold turkey is abruptly and completely ending all nicotine use without the use of quitting products.
Instead of getting excited and immediately deep-diving into how nearly all successful daily youth smokers succeeded, as reflected by Truth's website pages, Truth effectively suggests that nearly all successful adolescent ex-nicotine users picked the wrong method.
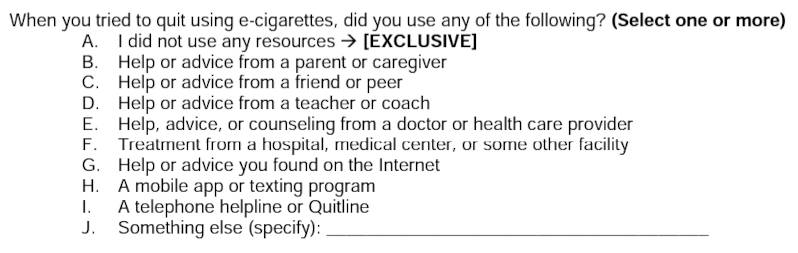
Putting the nation’s head in the sand, the 2021 and 2022 National Youth Tobacco Surveys did not ask any questions about any quit smoking method.
While question 28 asks about quitting vaping, the choices provided are method accompaniments (support, counseling, programs, apps, texting, or a quitline), not core methods such as cold turkey, gradual weaning, NRT, Chantix (varenicline), Zyban (bupropion), or Tabex or Desmoxin (cytisine), or switching/transfer to a different nicotine delivery product such as e-cigarettes, pouches, IQOS or smokeless tobacco.
That's like asking about hot dog or hamburger condiments, or pizza toppings, without knowing what they adorn.
A July 12, 2023 Truth page tells smokers that, "Quitting is difficult. It takes the average smoker 11 quit attempts before successfully quitting."
What it doesn't tell them is the actual lesson eventually self-discovered via the school of hard-quitting-knocks, and why that lesson can't be mastered before their first attempt ever.
How many Truth Initiative board members, are curious about the key or keys to successful cold turkey quitting, and how easy or hard identifying and sharing them would be?
While Truth deserves credit for a substantial role in the dramatic decline of youth smoking since 1998, since 2010 e-cigarette use has exploded. To its credit, Truth has worked hard to turn things around.
While facilitating successful adolescent nicotine dependency recovery is one of life’s greatest challenges, we won’t get there by ignoring analysis of what works and what doesn’t, or by Truth declaring a youth and young adult stop vaping text messaging intervention demonstrating “nonsignificant efficacy” at 6 months (see Figure 7) as being “effective.”
"This is Quitting" has tremendous potential. But it won't be realized by Truth allowing teen and young adult e-cig quitters to teach their peers what works and what doesn't. Although well intended, many shared tips are unsupported by science and at least one is likely to excite the neo-nic industry.
Hard to miss, "jt_deleeuw" advises young e-cigarette users and quitters to "Get rid of the vape and switch to nicotine pouches like zin, or snus." Following this advice would extend recovery, induce nicotine relapse if clean, and risk creating a dual user of both e-cigs and pouches.
Cancer & Primary Care
Back to Truth’s many suggestions that successful cold turkey quitting is rare, a 2021 study of 151 active smokers diagnosed with bladder cancer found that 115 made a quitting attempt with 65 (56%) being successful. Among the 65 successful quitters, 42 or two-thirds (66%) quit cold turkey.
A 2022 study of 186 mostly heavy long-term smoking patients diagnosed with head or neck cancer found that at six months 13 patients had died and 41 had quit smoking. Most, 51.2%, successfully quit cold turkey with 14% quitting via NRT.
What about less motivated quitters -- family practice patients?
A 2006 study analyzed patient smoking and quitting histories of Australian primary care physicians. Not only was cold turkey by far the most effective method -- doubling the success rate of nicotine gum, patch, and inhaler quitters -- it was by far the most productive in generating 1,942 of 2,207 former smokers, a mammoth 88% of all successful quitters.
Adult Quitters
Let’s look at peer-reviewed observational studies published in journals affiliated with two of Truth's most trusted partners, the Mayo Clinic and the National Cancer Institute (NCI), and a second unpublished NCI study.
Findings from a 2014 UK prospective population-level quitting study published in Mayo Clinic Proceedings found that "Compared with smokers using none of the cessation aids" at the 6-month follow-up ... "use of NRT bought over the counter was associated with a lower odds of abstinence (odds ratio, 0.68; 95% CI, 0.49-0.94)."
The vast majority of U.S. NRT sales are OTC. According to a 2023 FDA & CDC study, "over-the-counter nicotine replacement therapy sales totaled about $1 billion annually between 2017 and 2020." According to the study, in 2020, gum accounted for 52.7% ($511 million), lozenges accounted for 33.3% ($322 million), and patches accounted for 14.1% ($137 million) of OTC NRT sales.
Like the Truth website not telling teens how most teens successfully quit, a 2007 front-page WSJ article by a Pulitzer Prize-winning journalist featured findings from a non-published 2006 NCI survey.
The NCI found that among 8,499 quitters at least 25 years of age, 66% quit without the use of approved quitting products. Among 8,200 quitters providing 9-month data, non-medication quitters generated a slightly higher success rate (16%) than nicotine patch (14%), gum or lozenge (14%), bupropion (12%), or NRT combination quitters (12%).
Contrast Truth’s claim that “at most, only 3-5% can” to the NCI’s finding that “16% did.” As for productivity, 5,412 non-medication attempts generated roughly 866 successful quitters, compared to 2,588 approved product users generating, at most (using 14%), 362 quitters.
Likely the most robust population-level study yet, a 2017 study published in the Journal of the National Cancer Institute scrutinized data from 2,219 pharmaceutical aid users and nonusers participating in 2002-2003 and 2010-2011 TUS-CPS surveys.
Using propensity score matching for 12 potential confounders (age, sex, race-ethnicity, education, smoking intensity, nicotine dependence, previous quit history, self-efficacy to quit, smoke-free homes, survey year, and cessation aid use) they found “no evidence that use of varenicline, bupropion or nicotine replacement increased the probability of 30 days or more smoking abstinence at one-year follow-up."
The authors concluded that “The lack of effectiveness of pharmaceutical aids in increasing long-term cessation in population samples is not an artifact caused by confounded analyses. A possible explanation is that counseling and support interventions provided in efficacy trials are rarely delivered in the general population.”
BecomeAnEx
As found by a 2019 Truth study, by 2017, more than a third of all smokers were turning to the Internet for help quitting, representing more than 12 million US adults. BecomeAnEx is Truth's primary tool to help them.
According to a 2016 study co-authored by Truth, "BecomeAnEX assists users in setting a quit date, understanding their smoking habits and preparing to quit, selecting and using Food and Drug Administration–approved medications, and connecting with others for social support in the BecomeAnEX community."
"BecomeAnEX, a digital quit-smoking plan and online community of thousands of smokers and ex-smokers, has helped more than 800,000 people develop the skills and confidence to successfully quit," states a March 24, 2020 Truth press release.
Question. Is Truth saying that 800,000 BecomeAnEx users successfully quit?
I ask because according to a 2017 study co-authored by Truth employees, "a national mass media campaign and online advertising have resulted in over 800,000 registered users since the launch of the site" (2008).
Interestingly, the purpose of a 2020 study co-authored by Truth was to explore the influence upon NRT beliefs of 3,297 BecomeAnEx support group members exposed to posts discussing NRT.
The most widely held effectiveness beliefs? That NRT does not "double the chance of quitting compared to cold turkey" (76.3%), that "they do not work" (65.1%), and "the only way to quit is to go cold turkey" (63.5%).
What Truth has yet to study is the influence of its relentless and multifronted attacks on cold turkey upon the beliefs of 3 classes of nicotine-dependent visitors to the Truth Initiative and BecomeAnEx websites: (1) users undecided about a method; (2) users who have decided to go cold turkey and are in search of abrupt cessation insights; and (3) cold turkey quitters in the throws of withdrawal.
How effective is BecomeAnEx? While Truth pages created 05/17, 04/18, 11/18, 01/19, 02/19, 06/19, 01/20, 11/20, 03/22, and 03/23 claim that the BecomeAnEX program “quadruples a tobacco user's chance of quitting,” no study reference supporting this assertion is provided.
Unable to locate any study comparing BecomeAnEx to a non-BecomeAnEx control, I requested a source from Truth but no reply was received before publication.
PubMed is our nation's free science literature search engine. A Pubmed search of "BecomeAnEx" returns 21 papers, 17 of which were published on or before 2017. While none compare BecomeAnEx to a non-BecomeAnEx control, one shares a BecomeAnEx program success rate that may provide insight into the control group rate that Truth contends is being quadrupled.
While Truth links its 3-5% cold turkey quitting rate claim to 6-12 months, as shared in a 2016 study co-authored by Truth, "Of the 1337 BecomeAnEX users in this sample, 12.27% (164/1337) reported 30-day point prevalence abstinence at 3 months."
Pre-dating all claims, could it be that simple, that the foundation supporting Truth's many "quadruple" your chances assertions is that 12% divided by 3% = 4? If so, we have a rather glaring math problem.
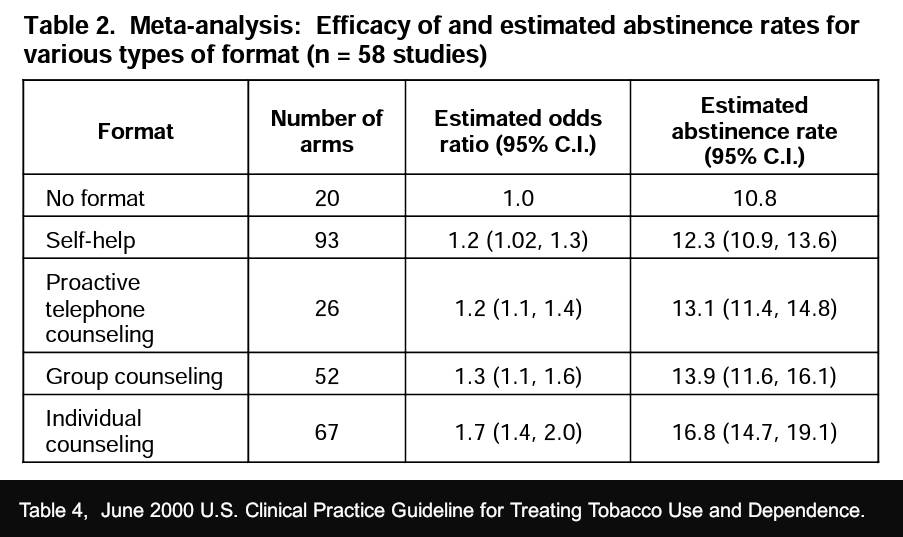
Again, although reflecting clinical efficacy among treatment seekers, not cold turkey observational effectiveness, Table 2 of the 2000 Guideline included 93 study arms in calculating a 6-month "self-help" success rate of 12.3%.
Slightly less, Table 6.11 from the 2008 Guideline Update used half as many arms (47) in calculating a 10.9% "self-help" rate. However, Table 6.26 found an average placebo arm rate of 13.8% (80 arms).
Financial Disclosures
While Truth continues to acknowledge a “Featured Partnership” with the Pfizer Foundation, having no actual conflicts disclosure page, Truth's financial ties to the quitting industry are unclear.
Why care? Why does it matter?
Professor Michel Siegel, a physician, tobacco control activist, and former employee of the CDC's Office of Smoking and Health titled his July 17, 2013 blog "Pfizer's 'Don't Go Cold Turkey' campaign highlights widespread misunderstanding of the scientific evidence on quitting."
According to Professor Siegel, "One of the greatest misconceptions in tobacco control is that the use of medication improves the chances of quitting compared to 'cold turkey' quitting."
"The scientific evidence shows clearly that spontaneous (unplanned) cold turkey quitting is more effective than planned, medication-assisted quitting. The evidence also shows that on a population basis, the overwhelmingly most successful method used to quit is cold turkey quitting."
"To make the statement that medication is more effective than cold turkey quitting, one would have to compare a group of smokers given medication to a similar group who are motivated to quit cold turkey. You cannot randomize people to quit cold turkey because it takes a sincere desire to do so and a high level of motivation," Siegel explains.
To the point, "It is easy to understand why Pfizer would misrepresent the science. But why is there such a high prevalence of misrepresentation of the data among anti-smoking groups and practitioners?" asks Siegel. "At least part of the answer, I believe, is the tremendous amount of funding that anti-smoking researchers and groups have received from Big Pharma."
While Truth is a 501(c)(3) non-profit that received $7.4 million in contributions during 2021, its Form 990 Schedule B does not disclose contributors and is annotated “restricted” as to both name and amount.
Truth is a national foundation established by the states. Given that Truth discourages cold turkey quitting in many of its publications, Truth should disclose its annual quitting industry contributions, expenditures, and partnerships, if any.
It’s Not Too Late
With a new CEO backed by a board that includes 3 “first, do no harm” physicians and 5 attorneys who recognize unfair and deceptive trade practices when they see them, what better time than now to demand complete, unfiltered, and accurate snapshots of U.S. adolescent, young adult, and adult nicotine dependency recovery and switching.
While there's no debate but that Truth substantially contributed to reducing youth smoking initiation to historic lows, young adults haven’t fared as well. According to a 2020 JAMA study, the “proportion of ever smokers who initiated cigarette smoking in early adulthood more than doubled between 2002 and 2018.”
To date, has Truth offered meaningful assistance to the millions of teens and young adults who fell through the cracks over the past 24 years? Frankly, we can and must do better.
Why be afraid to tell smokers the truth about quitting methods? If Truth hasn't yet discharged its 1998 MSA obligation to investigate and determine what works, how could it possibly develop the institutional confidence needed to openly acknowledge that clinical efficacy is almost always at odds with population-level effectiveness?
According to the 2008 Guideline Update, in that the Guideline's randomized trials occurred in research settings, "it is imperative that new research examine implementation of effective treatments in real-world clinical settings." Except for limiting real-world research to "clinical" settings -- a path utilized by less than 5% of quitters -- I couldn't agree more.
The alternative? I strongly suspect that history will judge us harshly. Eventually, creative researchers will figure out how to compute the harm and lives lost due to campaigns aimed at getting quitters to resist their quitting instincts. They may also produce findings as to the number of smokers who grew so frustrated with quitting that they switched and spent the balance of their lives as slaves to vaping or dual-use.
Does one size fit all? No. Does gradual stepped-down nicotine weaning perform better in highly supportive environments? All methods do. Might quitters suffering from chronic depression or other mental health issues benefit from medications and from having skilled providers on their cessation team? Absolutely!
But anyway it's cut, teaching smokers that quitting cold turkey is wrong, is wrong.
Harm reduction often claims that many smokers can’t quit. But is it true? Would it be as true if Truth dedicated as many pages to sharing the key to successful cold turkey quitting as it does in discouraging it?
When the money is gone, what will Truth’s nicotine dependency recovery legacy be? Stay tuned.
 John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," 6 peer-reviewed journal articles, and founder and director of Turkeyville, a 17,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com
John R. Polito received his JD from the University of South Carolina School of Law in 1985, where he graduated Wig & Robe. He is a former 3-pack-a-day thirty-year smoker and the 1999 founder of WhyQuit. A nicotine cessation educator since 2000, John mentored under Joel Spitzer for two decades, presenting more than 100 live nicotine dependency recovery programs modeled after Joel's programs. He is the author of "Freedom from Nicotine - The Journey Home," "Smart Turkey," 6 peer-reviewed journal articles, and founder and director of Turkeyville, a 17,000-member Facebook support group exclusively for cold turkey quitters. Email: johnpolito54@gmail.com

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}